Premenstrual tension syndrome manifests as cyclic behavioral, psychological, and physical symptoms related to the luteal phase of the menstrual cycle that may have oxidative stress bases. After ethical committee approval, our study enrolled sixty obese women having premenstrual tension syndrome (PTS) divided into younger age group (18-39 years) and older age (40-48 years) versus an age-matched healthy control group. Body mass index, serum oxidized LDL, serum total antioxidant capacity and serum angiopoietin-like protein-4 (ANGPL-4) were assessed in all women participating in this study. Some psychosomatic manifestations of premenstrual tension syndrome (mastalgia, aggression, and depression) were also assessed. Our study revealed that obese PTS women had significantly increased oxidized LDL (p<0.01) and angiopoietin-like protein-4 (p<0.01), while serum total antioxidant capacity was significantly decreased (p<0.01). Mastalgia, aggression, and depression significantly increased (p<0.001) in women having PTS. All that significantly improved upon using combined therapies including Metformin, Amiloride/ Hydrochlorthiazide, caloric restriction diet, walking exercise, Vitazinc or Royal vitamin G. Such combined therapies significantly decreased (p<0.001) the severity of all investigated psychosomatic symptoms that went in line with the normalization of serum biochemical parameters. Improved serum biochemical and oxidative stress parameters were better upon using combined therapies containing Royal vitamin G significantly (p<0.05) than combined treatments containing Vitazinc. In conclusion, obesity-related oxidative stress effectors are treatable factors in managing PTS. Combined therapies including Vitazinc or Royal vitamin G are promising pharmacological therapeutics for alleviating premenstrual tension syndrome. Fennel (Foeniculum vulgare Mill) is an interesting medicinal plant and a prophetic medicine remedy that treats obesity effects and treating many manifestations of premenstrual tension syndrome. Fennel is rich in antioxidant ingredients as anethol. Fennel helps treating various psychiatric conditions and we highly recommend using it in clinical psychiatry.
premenstrual tension syndrome, oxidative stress, psychosomatic manifestations, mastalgia, aggression, Royal vitamin G, Vitazinc
Increased oxidative stress and reduced antioxidant capacity may occur in premenstrual tension syndrome. Lipid hydroperoxide increased while total antioxidant capacity decreased in women having premenstrual tension syndrome [1].
Menses irregularities, painful menstruation, and symptoms of premenstrual tension syndrome are significantly associated with increased intake of calories, proteins, carbohydrates, and fat. Moreover, obesity worsens menstruation-related complications [2]. Moreover, serum levels of inflammatory markers, including interleukin (IL)-2, IL-4, IL-10, IL-12 and interferon (IFN)-γ were positively associated with menstrual symptoms severity and/or premenstrual syndrome. In a cross-sectional study that involved 277 women aged 18-30 years, total menstrual symptom score was positively associated with serum levels of IL-2, IL-4, IL-10 and IL-12. Affective menstrual symptom score was directly proportional to serum IL-2, while physical/behavioral symptom score was linearly related to levels of IL-4 and IL-12 [3-5].
Angiopoietin-like protein-4 has been demonstrated to affect vascular permeability, inflammation, and oxidative stress [6]. Angiopoietin-like protein-4 activity is associated with endothelial cell integrity, inflammation, oxidative stress, and lipid metabolism. Angiopoietin-like protein-4 is a regulator of oxidative stress. Some studies indicate that Angiopoietin-like protein-4 can protect the integrity of endothelial cells, while others have shown that it can be destructive to the endothelium, thereby leading to the initiation of atherosclerosis [7].
Metformin is a currently and widely used drug to reduce serum glucose and weight in diabetic and obese patients [8]. Metformin also suppresses obesity-associated inflammation via affecting macrophages [9].
Hydrochlorothiazide and Amiloride helped the long-term treatment of oedema of congestive heart failure [10].
Royal vitamin G capsules contain a combination of different multivitamins in addition to minerals, ginseng royal jelly, pollen, and di-methyl-amino-ethanol. Vitazinc Capsules includes a combination of vitamin E, vitamin A, and zinc. Both Royal vitamin G capsules and Vitazinc are commonly prescribed as tonics for treating different disease conditions.
Our study examined a possible relationship between obesity-induced oxidative stress markers (oxidized LDL and total antioxidant capacity) and some symptoms of premenstrual tension syndrome. This study also examined a possible therapeutic effect of using Hydrochlorothiazide, Amiloride, walking exercise, metformin, and caloric restriction for six months on the severity of inflammatory and psychosomatic features of premenstrual tension syndrome e.g., aggression, depression and mastalgia. We also investigated novel possible effects of the biochemical mediators e.g., angiopoietin-like protein-4 on premenstrual tension syndrome.
Study design
Sixty obese women diagnosed with premenstrual tension syndrome were categorized into two different age groups: younger (18-39 year) and older age groups (40 -48 year) versus the control group (non-obese women of the same age groups). A prior informed patients’ consent and ethical committee approval were performed from Faculty of Medicine, Tanta University, Egypt.
Pharmacological intervention
The study duration included six months of low caloric diet, daily walking exercise (half an hour regularly) and pharmacological medications (Amiloride hydrochloride/ Hydrochlorthiazide 5/50 mg, metformin, Vitazinc capsules and Royal vitamin G capsules) seven days before menstruation for six successive cycles.
Women’s assessment and investigated parameters
Body mass index and serum oxidized LDL, total antioxidant capacity, angiopoietin-like protein-4 (ANGPL-4) were evaluated for all subjects.
In addition, some psychosomatic manifestations were also evaluated before and after given treatments in the control group and in women having some manifestations of premenstrual tension syndrome. Assessed psychosomatic features included: mastalgia, aggression and depression.
Serum oxidized LDL assay
Oxidized LDL was assayed in serum of all women in the control and treatment groups using Oxidized LDL assay kit (Abcam, MA, USA) according to manufacturer’s instructions. Briefly, all reagents, samples and standards were prepared.
OxLDL standard or sample was added to the anti-OxLDL Antibody coated plate, covered, and incubated for 2 hours. at room temperature. Washing steps using wash buffer were done followed by adding diluted Biotinylated Anti-Human ApoB-100 antibody to each well followed by incubation for 1 hour at room temperature and washing. Streptavidin-Enzyme Conjugate was added to each well followed by incubation for 1 hour at room temperature followed by washing. Then, warm substrate solution was added to each well followed by incubation for 5-20 minutes at room temperature. Enzyme reaction was stopped upon adding stop solution to each well. Optical density value of each well was assayed at 520 nm using Biotek Synergy multimode microplate reader.
Total antioxidant capacity assay
Serum total antioxidant capacity was assayed using total antioxidant capacity assay kits (elabscience, TX, USA) according to manufacturer’s instructions. Briefly, fresh blood was collected and stood at 25° for 30 min to clot. Then, centrifugation was done at 2000 g for 15 min at 4°. In test tubes, buffer solution was added to serum. Chromogenic agent working solution and of ferric salt stock solution working solution were then added to both sample tubes and control tubes. Proper mixing was done, and they were allowed to react at 37° for 30 min. Ferric salt diluent, stop solution and clarificant were sequentially added. After fully mixing and standing for 10 min at room temperature, reaction liquid was added to 96 well microplates and measure the optical density value of each well at 520 nm using Biotek Synergy multimode microplate reader.
Serum angiopoietin-like protein 4 assay kits
Circulating Angiopoietin-like protein 4 levels were assayed (according to manufacturers’ instructions) using Human Magnetic Luminex Screening Assay (LXSAHM; R&D Systems, Inc. Minneapolis, MN, USA) on bio-plex200 platform (Bio-Rad, Hercules, CA, USA). The lower limits of detection were 86 pg/mL for Angiopoietin-like protein-4. Reaction liquid was added to 96 well microplates and optical density was measured using Biotek Synergy multimode microplate reader.
Assay of psychosomatic manifestations
Aggression was rated using The Overt Aggression Scale for Rating Aggression as previously reported [11]. Mastalgia rating was done using the new breast pain chart [12]. Depression was assessed using depression-anxiety rating scale as reported previously [13].
Quantitative assessment and statistics
Data were collected and analyzed statistically using SPSS software (version 13.00; SPSS Inc., Chicago, Illinois, USA). Mean ±SD were presented. One-way ANOVA analysis of variance was done. P values indicates significance differences from control group (*p <0.05, ** indicates p< 0.01 and *** indicates p< 0.001). #, # # and # # # indicate significance differences among different treatment conditions within the same group (# p <0.05, # # indicates p< 0.01 and # # # indicates p< 0.001).
Effects of obesity and combined therapies on body mass index and psychosomatic manifestations
Body mass index was estimated for all women (having premenstrual tension syndrome) and the control group (non-obese women lacking premenstrual syndrome). Body mass index increased significantly (p<0.05) in women having premenstrual tension syndrome (before treatment) and significantly decreased later (p<0.05) upon using the combined therapy regimen for six consecutive months (Figure 1). There was no significant decrease or difference in decreasing body mass index among women having premenstrual tension syndrome and taking either Vitazinc or Royal vitamin G (Figure 1).
Figure 1. Effects of obesity and combined therapies on body mass index.
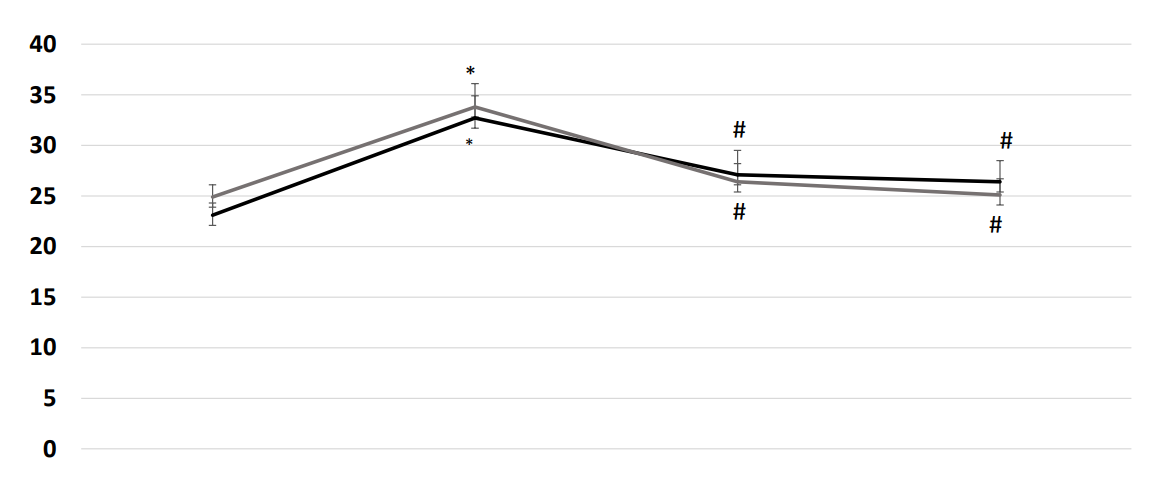
Body mass index was estimated for all women participating in the study: control groups and obese women (having premenstrual tension syndrome). Obesity was significant (p<0.05) in women having premenstrual tension syndrome at the beginning of our study and decreased later upon using the combined therapy regimen for six consecutive months.
Effects of obesity and combined therapies on serum oxidized LDL
Compared to the control group, serum oxidized LDL significantly increased in obese females (of both age groups) (p<0.01). Combined treatment using (Metformin, Amiloride/ Hydrochlorthiazide, Vitazinc, caloric restriction diet, and half an hour of walking exercise per day) significantly decreased serum total antioxidant capacity (p<0.01). Moreover, Combined treatment using Metformin, Amiloride/ Hydrochlorthiazide, Vitazinc or Royal vitamin G, caloric restriction diet, and half an hour of walking exercise per day) significantly decreased serum oxidized LDL that was corresponding to decreased body mass index. (Figure 2).
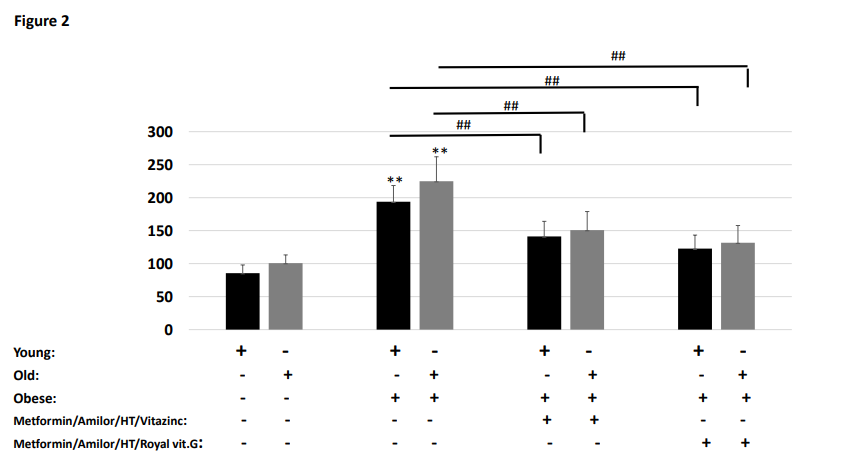
Figure 2. Premenstrual tension syndrome was significantly associated with increased serum oxidized LDL. This significantly decreased upon using combined therapies.
Effects of obesity and combined therapies on serum total antioxidant capacity
Compared to control group, serum total antioxidant capacity significantly decreased in obese females (of both age groups) (p<0.01). Combined treatment using (Metformin, Amiloride/ Hydrochlorthiazide, Vitazinc, caloric restriction diet, and half an hour of walking exercise per day) significantly increased serum total antioxidant capacity (p<0.05) to a better extent than combined therapy including Vitazinc. Resultant significant increase in total antioxidant capacity (Figure 3) was corresponding to decreased body mass index.
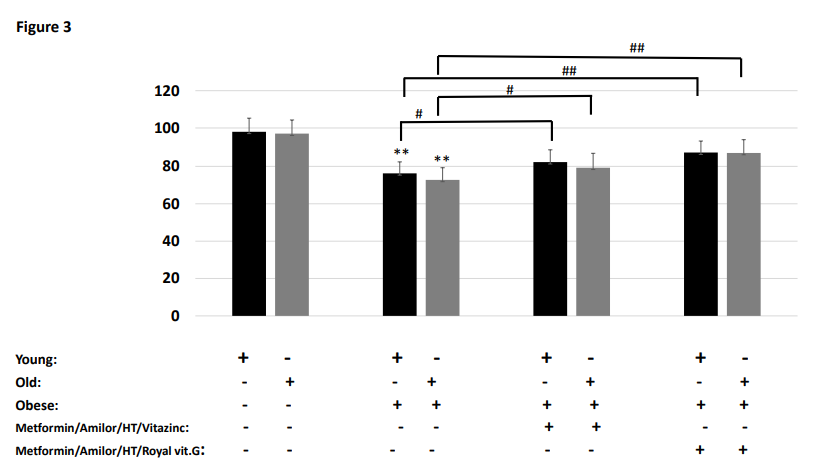
Figure 3. Premenstrual tension syndrome was significantly associated with decreased serum total antioxidant capacity. This significantly increased upon using combined therapies.
Effects of obesity and combined therapies on serum Angiopoietin-like protein-4 (ng/ml) and psychosomatic manifestations
Our data revealed also that serum Angiopoietin-like protein-4 was significantly higher in obese women (in both age groups, p<0.01) compared to their controls (non-obese women of the same age group) and in older healthy women than in young healthy women (Figure 4). Combined therapies using (Metformin, Amiloride/ Hydrochlorthiazide, Vitazinc, caloric restriction diet, and half an hour of walking exercise per day) significantly decreased serum Angiopoietin-like protein-4 to near normal values (p<0.01) (Figure 4). Combined therapy using royal vitamin G decreased serum Angiopoietin-like protein-4 more significantly than combined treatment using Vitazinc (p<0.05) (Figure 4). That was also associated with marked improvement of the investigated psychosomatic manifestations (mastalgia, aggression and depression) (Figures 5A-C).
Figure 4. Effects of obesity and combined therapies on serum Angiopoietin-like protein-4 (ng/ml).
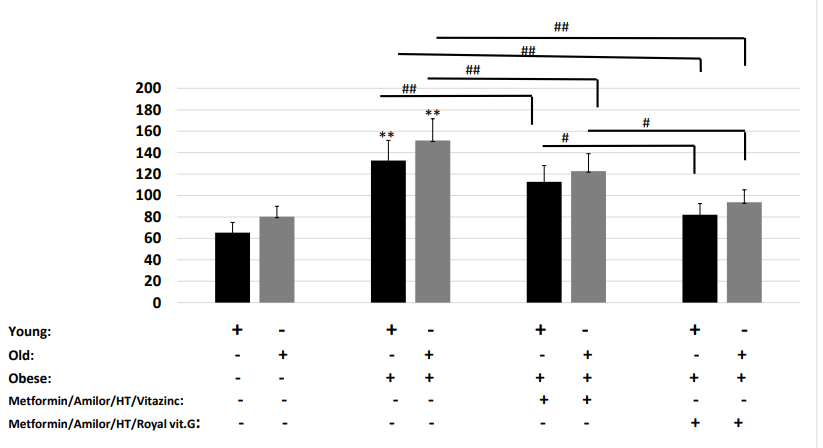
Serum Angiopoietin-like protein-4 was significantly higher in obese women (in both age groups, p<0.01) compared to their controls (non-obese women of the same age group) and in older healthy women than in young healthy women. Moreover, our data confirmed that combined treatments using (Metformin, Amiloride/ Hydrochlorthiazide, Vitazinc, caloric restriction diet, and half an hour of walking exercise per day) significantly decreased serum Angiopoietin-like protein-4 to near normal values (p<0.01). Combined therapies using Royal vitamin G decreased serum Angiopoietin-like protein-4 more significantly than combined treatment using vita zinc (p<0.05).
Figure 5. Effects of obesity and combined therapies on psychosomatic manifestations of premenstrual tension syndrome.
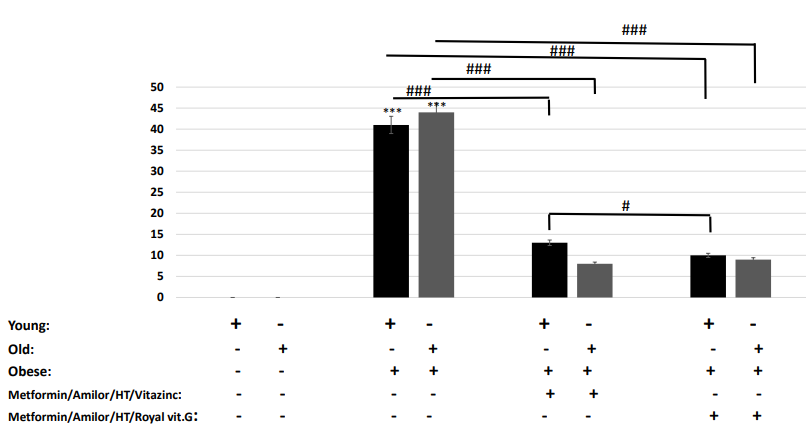
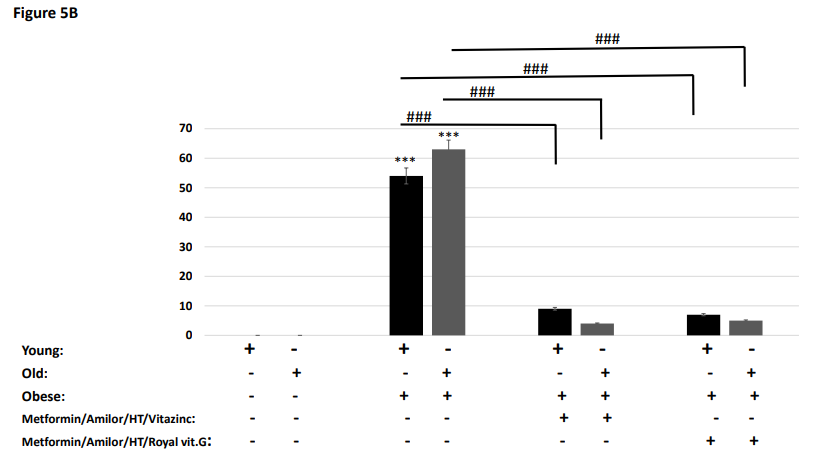
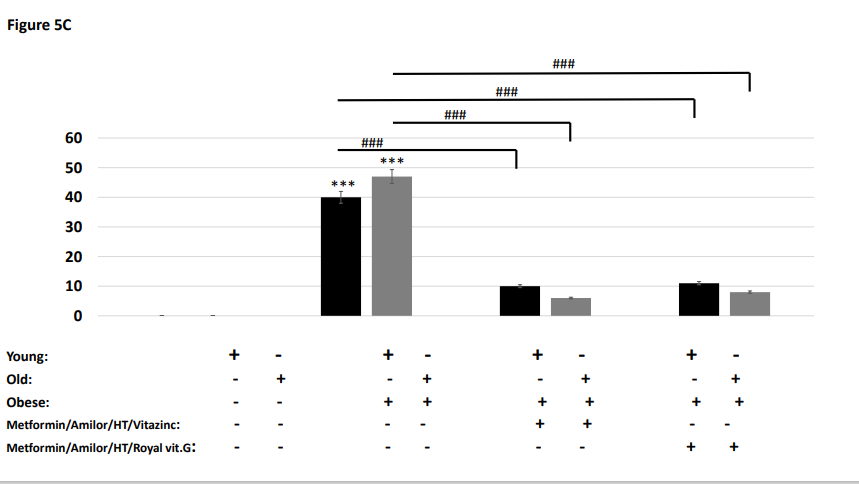
A-C. Obesity was associated with increased mastalgia, aggression and depression in both young and old obese women having premenstrual tension syndrome (p<0.001). Both combined treatment regimens (containing either Vitazinc or Royal vitamin G) significantly decreased mastalgia, aggression and depression in obese women having premenstrual tension syndrome (p<0.001). Combined therapies using Royal vitamin G significantly decreased these symptoms more than same combined therapies containing Vitazinc (p<0.05).
Effects of obesity and combined therapies on oxidative-stress-related psychosomatic manifestations
Mastalgia increased significantly (p<0.001) in obese subjects of both age groups compared to the healthy controls (Figure 5A). Combined treatments using (Metformin, amiloride/ Hydrochlorthiazide, caloric restriction diet, and half hour of walking exercise a day) with either Vitazinc or Royal vitamin G caused a significant decrease in mastalgia occurrence (Figure 5A). A significant improvement was also observed between vitazinc-containing combined therapies and Royal vitamin G-containing combined therapies (p<0.05) in the older age group but not in the younger age group (Figure 5A). Such improvement was in favour of combined therapy including royal vitamin G.
Aggression increased significantly (p<0.001) in obese subjects of both age groups (Figure 5B). Combined treatments including either Vitazinc or Royal vitamin G caused a significant decrease in aggression occurrence (Figure 5B). No significant difference was observed between Vitazinc-containing combined therapy and Royal vitamin G-containing combined therapy (Figure 5B).
Depression increased significantly (p<0.001) in obese subjects of both age groups (Figure 5C). Combined treatment including either Vitazinc or royal vitamin G caused a significant decrease in depression occurrence (Figure 5C). No significant difference was observed between Vitazinc-containing combined therapy and royal vitamin G-containing combined therapy (Figure 5C).
Obesity is associated with increased oxidative stress and related effects. Obesity is accompanied by the formation of oxygen free radicals. Rowicka, et al. reported that serum total oxidant concentrations were significantly higher while total antioxidant capacity concentration was significantly lower in obese children. Oxidative stress index was higher in obese subjects compared to control group. Median CRP value was higher and HDL cholesterol levels were lower in obese children. A significant negative correlation was reported between total antioxidant capacity and oxidized LDL concentrations in obese children. Obesity duration was positively correlated with total oxidant concentrations levels [14]. Dietary total antioxidant capacity was reported to be inversely associated with depression, anxiety, and some oxidative stress biomarkers in postmenopausal women. Serum malondialdehyde level (a lipid peroxidation product denoting presence of a harmful oxidative stress) was significantly lower in subjects having highest dietary total antioxidant capacity. In addition, serum total antioxidant capacity level was significantly higher in subjects taking high dietary total antioxidant capacity. Total antioxidant capacity was inversely and independently related to depression [15].
A strong linear relationship was reported between increased body mass index and premenstrual tension syndrome. For each one kg/m2 increase in body mass index, a 3% increase in premenstrual tension syndrome risk significantly occurs. Body mass index was positively associated with specific symptoms, including swelling of extremities, backache, and abdominal cramping. Decreasing body weight may be vital for preventing development of premenstrual tension syndrome [4].
Interestingly, our data confirmed that combined treatments including Vitazinc helped a significant decrease in body mass index that conferred psychosomatic health benefits with associated improvements in mastalgia, aggression and depression. In addition, combined treatments including Royal vitamin G also caused a significant decrease in body mass index to near normal values (Figure 1) that consequently had associated improvements in mastalgia, aggression and depression) (Figures 5A-C).
In women with premenstrual tension syndrome, arterial stiffness significantly increased during the luteal and menses phase. There was reported significant interactions between premenstrual syndrome and changes in arterial stiffness and blood pressure [16]. Diastolic blood pressure was reported to be elevated in young adult women having premenstrual tension syndrome [4]. This is in exact agreement with our data where premenstrual tension syndrome is associated with significantly increased serum oxidized LDL that significantly decreased with combined therapies (Figure 2). Consistent with that, our data also reported a significant decrease in total antioxidant capacity in women having premenstrual tension syndrome that significantly increased with combined therapies (Figure 3).
Increased serum Angiopoietin-like protein-4 was significant in women having premenstrual tension syndrome. Our data revealed that serum Angiopoietin-like protein-4 increased with obesity and decreased significantly with combined treatments using either vitazinc or royal vitamin G (Figure 4).
Mastalgia, aggression and depression increased significantly (p<0.001) in obese subjects having premenstrual tension syndrome of both age groups compared to controls (Figure 5A-C). Combined treatments having Vitazinc or Royal vitamin G caused a significant decreases in mastalgia, aggression and depression (Figure 5A). A significant better effect (in decreasing mastalgia) was gained after using Royal vitamin G-containing combined therapy than after using Vitazinc-containing combined therapies (p<0.05) in the older age group but not in the younger age group (Figure 5A-C).
Fennel (Foeniculum vulgare mill) is an interesting medicinal plant and a prophetic medicine remedy that appears to be very promising in maintaining women’s health, counteracting obesity effects and treats many manifestations of premenstrual tension syndrome. Fennel is a valuable plant in the management of women's health. Fennel is rich in antioxidant ingredients as anethol [17]. Fennel can be looked at as an excellent medicinal plant for treating various psychiatric conditions and we highly recommend using it in clinical psychiatry [18]. Topical and vaginal fennel extract (5%) exhibited good efficacy in treating sexual disorders, vaginal atrophy, and hirsutism. Results of many clinical studies introduce fennel as a valuable medicinal plant in managing women's ailments [17]. Interestingly, fennel is vital for postmenopausal women. Fennel is important in relieving the vasomotor symptoms, vaginal itching, dryness, dyspareunia (painful marital relation), sexual function, sexual satisfaction, and sleep distribution for menopausal women. fennel exerts potent oestrogenic effects as fennel contains phytoestrogens. In female rats, oral administration of the fennel extract for 10 days led to vaginal cornification and oestrus cycle. Fennel oil was reported to exhibit estrogenic activity, promote menstruation, and alleviate the symptoms of female climacteric, and increase libido [19].
This study concluded that premenstrual tension syndrome has oxidative stress bases (in addition to its inflammatory bases [20]) that may enhance its psychosomatic symptoms. Using combined pharmacological and non-pharmacological therapies eased decreasing obesity and psychosomatic manifestations. Combined therapies containing Royal vitamin G did better than those containing Vitazinc in alleviating psychosomatic manifestations of premenstrual tension syndrome. Fennel may be promising in treating many psychiatric and gynecological issues and psychosomatic manifestations.
The authors are grateful to deanship of Scientific Research in Taibah University for kindly supporting the research facilities to achieve that project.
- Duvan CI, Cumaoglu A, Turhan NO, Karasu C, Kafali H (2011) Oxidant/antioxidant status in premenstrual syndrome. Arch Gynecol Obstet 283: 299-304. [Crossref]
- Taheri R, Ardekani FM, Shahraki HR, Heidarzadeh-Esfahani N, Hajiahmadi S (2020) Nutritional Status and Anthropometric Indices in relation to Menstrual Disorders: A Cross-Sectional Study. J Nutr Metab 2020: 5980685. [Crossref]
- Bertone-Johnson ER, Hankinson SE, Willett WC, Johnson SR, Manson JE (2010) Adiposity and the development of premenstrual syndrome. J Womens Health (Larchmt) 19: 1955-1962. [Crossref]
- Bertone-Johnson ER, Houghton SC, Whitcomb BW, Sievert LL, Zagarins SE, et al. (2016) Association of Premenstrual Syndrome with Blood Pressure in Young Adult Women. J Womens Health (Larchmt) 25: 1122-1128. [Crossref]
- Bertone-Johnson ER, Ronnenberg AG, Houghton SC, Nobles C, Zagarins SE, et al (2014). Association of inflammation markers with menstrual symptom severity and premenstrual syndrome in young women. Hum Reprod 29: 1987-1994. [Crossref]
- Zolkiewicz J, Stochmal A, Zaremba M, Hoffmann A, Czuwara J, et al (2021) Serum concentration of angiopoietin-like protein 4 in patients with systemic sclerosis. Pol Merkur Lekarski 49: 28-31. [Crossref]
- Xu L, Guo ZN, Yang Y, Xu J, Burchell SR, et al. (2015) Angiopoietin-like 4: A double-edged sword in atherosclerosis and ischemic stroke? Exp Neurol 272: 61-66. [Crossref]
- Seifarth C, Schehler B, Schneider HJ (2013) Effectiveness of metformin on weight loss in non-diabetic individuals with obesity. Exp Clin Endocrinol Diabetes 121: 27-31. [Crossref]
- Jing Y, Wu F, Li D, Yang L, Li Q, et al. (2018) Metformin improves obesity-associated inflammation by altering macrophages polarization. Mol Cell Endocrinol 461: 256-264. [Crossref]
- Viherkoski M, Huikko M, Varjoranta K (1981) The effect of amiloride/hydrochlorothiazide combination vs furosemide plus potassium supplementation in the treatment of oedema of cardiac origin. Ann Clin Res 13: 11-15. [Crossref]
- Herpertz SC, Matzke B, Hillmann K, Neukel C, Mancke F, et al. (2020) A mechanism-based group-psychotherapy approach to aggressive behaviour in borderline personality disorder: Findings from a cluster-randomised controlled trial. B J Psych Open 7: e17.
- Gautam S, Srivastava A, Kataria K, Dhar A, Ranjan P et al. (2016) New Breast Pain chart for Objective Record of Mastalgia. Indian J Surg 78: 245-248. [Crossref]
- Badrasawi MM, Shahar S, Abd Manaf Z, Haron H (2013) Effect of Talbinah food consumption on depressive symptoms among elderly individuals in long term care facilities, randomized clinical trial. Clin Interv Aging 8: 279-285. [Crossref]
- Rowicka G, Dylag H, Ambroszkiewicz J, Riahi A, Weker H, et al. (2017) Total Oxidant and Antioxidant Status in Prepubertal Children with Obesity. Oxid Med Cell Longev 2017: 5621989. [Crossref]
- Abshirini M, Siassi F, Koohdani F, Qorbani M, Mozaffari H, et al. (2019) Dietary total antioxidant capacity is inversely associated with depression, anxiety, and some oxidative stress biomarkers in postmenopausal women: a cross-sectional study. Ann Gen Psychiatry 18: 3. [Crossref]
- Stamatelopoulos KS, Georgiopoulos G, Papaioannou T, Lambrinoudaki I, Kouzoupis A, et al. (2012) Can premenstrual syndrome affect arterial stiffness or blood pressure? Atherosclerosis 224: 170-176. [Crossref]
- Mahboubi M (2019) Foeniculum vulgare as Valuable Plant in Management of Women's Health. J Menopausal Med 25: 1-14. [Crossref]
- Delaram M, Kheiri S, Hodjati MR (2011) Comparing the Effects of Echinophora-platyloba, Fennel and Placebo on Pre-menstrual Syndrome. J Reprod Infertil 12: 221-226. [Crossref]
- Badgujar SB, Patel VV, Bandivdekar AH (2014) Foeniculum vulgare Mill: a review of its botany, phytochemistry, pharmacology, contemporary application, and toxicology. Biomed Res Int 2014: 842674. [Crossref]
- Mariah RM, El-Dardiry SA, Mahmoud HA, Mabrouk MM, El-Dardiry NA et al. (2022) Effects of obesity-related inflammator,y markers on psychosomatic manifestations of premenstrual tension syndrome: towards better therapeutic outcomes. SVU-IJMS 5: 11-25.