Abstract
A search was performed using four databases; Medline via PubMed, Cochrane, Scopus and ScienceDirect for relevant randomized controlled trials conducted from 2012 to 2025. The Jadad modified scale was used to assess risk of bias of included studies. Two reviewers independently screened, data extracted and quality assessed the studies.
Out of 216 articles, 10 relevant unique articles were found eligible and selected for the systematic review. A total of 1984 teeth were assessed of which 800 teeth were restored using HT. Four comparisons were evaluated; The HT showed similar results when compared with the conventional treatment using stainless steel crowns. However, it showed better success rates when compared to conventional treatment using standard materials, atraumatic restorative treatment and non-restorative caries control.
The HT appears to be a successful method for managing caries in primary teeth, particularly for proximal or multi-surface dentine lesions. It is well-tolerated by children and acceptable to parents, with mild adverse effects reported.
Keywords
hall technique, preformed metal crowns, primary molars, caries treatment, treatment outcome
Introduction
Minimally invasive dentistry is an aspect of restorative dentistry that tends to preserve the tooth structure and maintain the viability of the pulp [1]. In the past few years, the approach to managing carious lesions changed from traditional surgical treatments to biological treatments; “prevention of extension “instead of “extension for prevention” to give the tooth a better healing potential [1].
So knowing that tooth decay is a multifactorial disease, the biological treatment approach focuses on arresting the progression of the carious lesion by disorganizing the responsible ecosystem with less or even without surgical treatment, on the basis that no restorative material is better than the natural tooth structure [2,3]. Supporting this concept, the Hall technique (HT) emerged as an ultra-conservative method for treating carious primary molars [4].
This technique consisted of placing a stainless steel crown on a decayed deciduous molar with dentinal carious lesions without the need for anaesthesia, caries removal or, tooth preparation [4]. This method was first introduced by Doctor Norna Hall in 1998 and was not commonly known until recently, in the last few years HT was widely used by pediatric dentists as a pain-free alternative to conventional treatment, more accepted in children [5,6]. This systematic review aims to evaluate the effectiveness of HT in treating carious primary molars.
Materials and methods
Review question
The review question was: Is the HT efficient for treating carious primary molars?
This question was formulated using the PICOS format, including: Population: Carious asymptomatic primary molars with vital pulp. Intervention: HT using stainless steel crowns (SSC). Comparison: Atraumatic Restorative Treatment (ART), Non-Restorative Caries Treatment (NRCT), Conventional Treatment (CT) followed by restorations (Drill and fill), Silver Diamine Fluoride (SDF). Outcomes: The outcomes of interest were success of the treatment, minor failures or major failures, the cited items were defined as the following: success: maintained tooth with the absence of clinical signs of any pulpal pathology, Tooth exfoliated without the occurrence of any kind of failures. Minor failure: Caries progression (New/secondary caries), restoration failure (Loss/perforation with restorable tooth), signs of reversible pulpitis, no signs of infection/no endodontic treatment or extraction required. Major failure: Signs of irreversible pulpitis/infection, restoration loss with unrestorable tooth, tooth needs endodontic treatment or extraction. Studies: Randomised controlled trials.
The eligibility criteria
This review includes Randomised controlled trials, at least 12 months follow-up, studies on primary teeth, Asymptomatic carious lesions with vital pulp, Studies comparing the HT with other caries treatment methods, including the removal of decayed tissues with hand instruments or a dental handpiece with filling restoration, Pediatric patients (age ≤ 14 years old), Studies on humans in English or French language.
Search strategy
A systematic search covering the period from 2012 to 2025 was conducted using four databases: Medline via PubMed, ScienceDirect, Scopus and Cochrane library. An initial search was performed in September 2024 and a subsequent one was conducted in March 2025. For each database, a search plan was developed using the Boolean operators (AND, OR). The following MeSH terms were used: “Hall Technique”, “Hall crown”, “Molar”, “tooth, deciduous”, “primary teeth”, "dental caries”, “crowns”, “stainless steel”. Appropriate search strategies with identical keywords were developed for Scopus and ScienceDirect. The used keywords are summarised in Table 1.
Databases |
Search strategy |
Results |
Pubmed |
dental caries[MeSH Terms] AND crowns[MeSH Terms] AND (tooth, deciduous[MeSH Terms] OR Molar[MeSH Terms]) |
24 |
Science Direct |
(("hall technique") OR ("hall crown")) AND (dental caries) AND (primary teeth) |
24 |
Scopus |
1/("Hall technique") AND ("Dental caries" ) AND ( "Primary Teeth" )
2/ ("stainless steel" AND "crowns") AND ("Dental caries") AND ("tooth, deciduous" OR "Molar" ) |
123 |
Cochrane Library |
#1 Tooth, Deciduous
#2 Molar
#3 Crowns
#4 Stainless Steel
#5 Dental Caries
#6 #1 OR #2
#7 #3 OR #4
#8 #6 AND #7 AND #5 |
45 |
Table 1. Search strategy
Study selection
Three steps were used in the study selection process. To start, only the study titles were taken into account, excluding any references that were obviously unrelated. Then, the screening of the abstracts of the remaining studies from phase 1. Irrelevant references were excluded based on their abstracts. At this stage, a manual search was performed. Finally, full articles were reviewed to verify if they fit all the inclusion criteria above. The literature selection was done by three authors independently. Any disagreements on study inclusions, quality assessment, or data extraction were resolved by discussions. The authors of the included articles were contacted to obtain information on unclear or missing data. The electronic search results were then imported into the EndNote20 software and duplicated records were discarded.
Data extraction process
A pilot-tested spreadsheet was used for data extraction it was performed by the three reviewers. The following elements were considered: author, year, and type of the study, number of participants, age of the participants, number of teeth, gender, intervention and follow-up duration. The protocol and the post-treatment outcomes were extracted and detailed in two separate spreadsheets.
Quality assessment of the included studies:
The “Modified Jadad Scale “was used to identify the risk of bias in randomized controlled trials.
Results
Selection of studies
A total of 2016 articles were identified in the initial search. After removing duplicates, 155 articles remained. Three reviewers independently screened the titles, abstracts, and full texts. Following the title screening, 123 references were excluded. Of the 32 articles remaining, 15 were retained after reviewing the abstracts. No additional eligible studies were found during the manual search. After the full-text screening, all 10 articles were deemed eligible for inclusion in this systematic review (Figure 1).
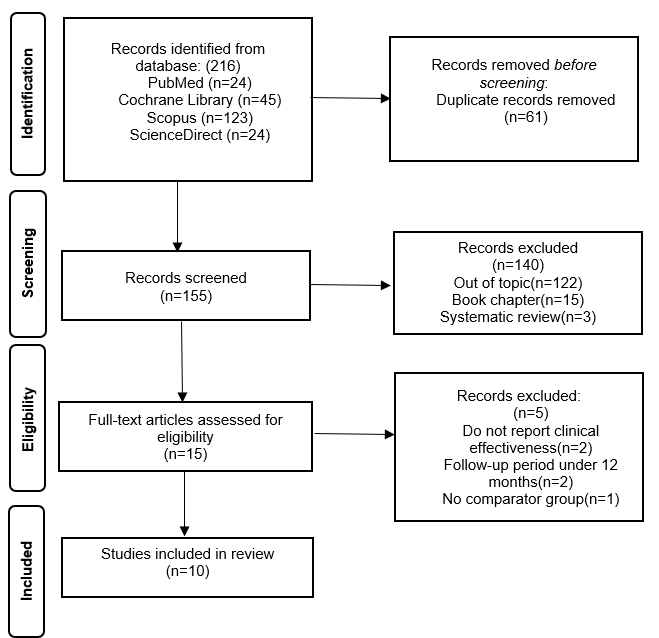
Figure 1. Search strategy flow chart
Data extraction
The characteristics of the included studies are described in Table 2, treatment protocols are listed in Table 3 and clinical and radiographic outcomes are listed in Table 4.
Table 2. Description of the selected studies.
Table 3. Treatment protocols of the selected studies
Table 4. Clinical and radiographic post-treatment outcomes
Table 5. Evaluating the risk of bias of the included studies according to Jadad modified scale
Characteristics of included studies
In this review, all the included studies were randomised controlled trials. The earliest included article was published in 2015 [7] and the most recent one was published in 2024 [8]. The controlled trials were conducted in the following countries: UK, Germany, Sudan, Brazil, Iran, Turkey, New Zealand, Nigeria and Lithuania.
The number of teeth included in the trials ranged from 46 [9] to 570 [10]. The majority of the controlled trials (90%) included patients with a high risk of developing new caries. Four studies were conducted on primary molars with occluso-proximal lesions. Six studies were conducted on primary molars with single or multi-surface carious lesions. Six of ten studies included cavities with ICDAS (International Caries Detection and Assessment System) codes varying from 3 to 5 while the remaining four articles did not mention the cavities’ depth.
The 10 studies compared the HT with other 3 minimally invasive treatments (ART, modified ART, NRCT) and with conventional treatment: HT vs. ART in 1 study [11], HT vs. mART in 1 study [12], HT vs. NRCT in two studies [8,13] and HT vs. CT in nine studies [7-10,12-16].
Reported protocols for the different interventions
For the HT group no caries eviction was performed in nine studies, the remaining study did not communicate the cavity preparation protocol [12]. Four trials specified the removal of only food and debris from the cavity. For the ART procedure, plaque removal followed by cavity widening and selective caries removal has been performed using hand instruments (Dental Hatchet with an excavator) whereas for the modified ART, high and low-speed burs were used respectively for the enamel margin and selective soft dentine removal [11,12]. In the NRCT groups, the overhanging enamel was removed using high-speed bur then the cavity was cleaned with a rotary bristle brush and fluoride varnish (22.600 ppm) [8,13]. For the CT groups, seven studies precised complete caries removal with rotary instruments [7-9,12-15], while in two studies [10,16] selective carious excavation was performed in order to avoid pulp exposure.
Reported clinical outcomes
• Comparison of HT with ART/modified ART:
Two trials compared HT with ART and modified ART. HT had higher success rates than both techniques. At one year follow up the HT showed a higher success rate (98%) compared to the mART success rate (48%). None of the restored molars with the HT recorded minor failures while 18% of those treated with mART presented minor failures. Major failures were recorded in one HT restoration (2%) compared to 34% in mART restorations. At 3 years follow-up, the HT showed higher success rates (96.9%) compared with the ART (49.23%).
• Comparison of clinical outcomes of HT with NRCT:
After two years, HT showed a higher success rate (93.8%) compared to NRCT (42.5%). None of the restored molars with the HT recorded minor failures while 24.2% of those treated with NRCT presented minor failures. Major failures were recorded in 6.2% of HT restorations compared to 33.3% in NRCT restorations.
After two and a half years HT showed a higher success rate (92.5%) compared to NRCT (70%). Minor failures reported for the HT were only 5% (1 restoration lost and 1 revealed new caries). NRCT showed 21% of minor failures distributed as follows: seven molars with new/secondary caries and two molars with signs of reversible pulpitis. One Molar treated with HT reported major failure compared to four molars treated with NRCT.
• Comparison of clinical outcomes between HT and the conventional treatment:
Nine trials compared clinical outcomes of HT with conventional treatment. Seven studies showed success rates of HT overcoming the conventional treatment. Two studies showed insignificantly higher success rates of the CT with SSC compared to the HT [12, 14].
Quality assessment of the included studies
The Jadad modified scale was used to evaluate the risk of bias in the included studies. All evaluated articles reported clearly focused questions, inclusion and exclusion criteria, data regarding dropouts, and statistical analysis methods. The majority succeeded in reporting the randomization methods except for Kaptan A and Korkmaz E that did not report clearly the randomization methods [15]. For Boyd, et al. trial, an allocation bias arising from the randomization process was detected [10]. It was due to the baseline differences between intervention groups that suggested a problem. Innes, et al., Kaptan A and Korkmaz E and Ayedun, et al. used a split-mouth design in their studies [7,9,15]. This design is interesting as it removes considerable inter-individual differences from the treatment efficiency evaluation. Furthermore, most articles did not report clear data related to blinding methods, with a complete lack of blinding in seven trials [7-9,11,13,15,16] which can result in a selection bias. Blinding operators, participants and outcome reviewers were not possible because compared treatments were different. Accordingly, knowing that the intervention technique was not blinded, unconscious bias might be introduced as dentists may use the HT with hesitation on the assumption that CT would give better results (Table 5).
Discussion
The majority of trials included teeth with ICDAS codes ranging from 3 to 5, which correspond to a localised enamel breakdown without dentine involvement to a distinct cavity with visible dentin. These codes indicate carious lesion progression extending to, or less than, halfway into the dentine [17]. Boyd DH et al. investigated the impact of caries depth on clinical outcomes [10]. The study concluded that, after two years of follow-up, there was no significant difference in the success rates of various interventions based on the baseline caries depth (ICDAS codes 3 to 5). Similarly, Santamaria et al. reported comparable findings; their trial revealed no significant correlation between cavity depth (ICDAS codes 3 to 5) and failure rates after two and a half years of follow-up [13]. A histological study on pulpal inflammation in primary molars demonstrated that when caries depth was less than halfway into the dentine, there was no significant difference in the status of pulp inflammation [18].
Ebrahimi, et al. reported a significant variation in outcomes depending on the affected surfaces [12]. The ART group demonstrated higher survival rates with single-surface lesions compared to multi-surface restorations. The study also found that the survival rates of the HT and CT with SSC were not influenced by the affected surfaces of carious molars. Both techniques showed impressive success rates, with 98% for HT and 100% for CT in managing multi-surface caries. In contrast, mART showed approximately 50% failure rates in molars with multi-surface lesions [12]. Further studies have indicated that different restorative materials do not perform equally across various affected sites [19,20]. The American Academy of Paediatric Dentistry recommends the use of SSC for multi-surface lesions to achieve better clinical outcomes [21].
Various techniques were employed in the included studies. In the CT procedure, complete caries removal was performed in most trials. For ART and mART, interventions involved selective caries removal. In contrast, techniques such as HT and NRCT involved no caries removal.
Notably, interesting findings were revealed when comparing different levels of carious tissue removal. No significant difference in success rates was found when comparing the HT, which included no caries removal, to CT with complete caries removal followed by SSC restoration [14,15]. A long-term follow-up trial even reported that the HT (no caries removal) achieved better success rates than the CT (complete caries removal) [7]. Evidence suggests that sealing-in caries has advantages over complete caries removal. Boyd, et al. found that the selective caries removal approach not only prevents pulp exposure and preserves tooth structure but also reduces treatment time and simplifies the intervention [10]. Consequently, the authors concluded that selective carious tissue removal improves clinical outcomes. Ultimately, the HT challenges invasive methods for restoring decayed primary molars, demonstrating significantly lower failure rates compared to conventional treatment.
The longevity of restoration in primary teeth depends on the selected material. Regardless of the chosen technique, conventional or Hall, SSCs demonstrated the highest survival rates for restoring decayed primary molars. In addition to providing full coverage that enhances isolation, sealing with glass ionomer supports lesion remineralisation and minimises microleakage [9,10,12,14,15].
The reported results from the included studies revealed that the HT, with a success rate of 98% outperformed other minimally invasive treatments such as modified ART and mART, which achieved approximately 50% success rates after one year of follow-up. Based on these outcomes, Ebrahimi, et al. recommended replacing ART with the HT in deprived communities, suggesting it should become the new “gold standard” intervention for uncooperative children due to its simplicity and reduced treatment time [12].
When comparing NRCT with CT using compomer restorations, no significant difference in outcomes was found. Given the comparable results, the authors questioned the necessity of surgical caries removal and the placement of restorative materials, instead advocating for minimally invasive approaches such as HT and NRCT [13]. Further studies described the effectiveness of NRCT and acceptable outcomes were reported with good survival rates of treated teeth [20]. Whereas, the treatment highly depended on the patient caregiver’s ability to maintain good plaque control, adhere to a healthy diet, and attend regular follow-ups to prevent and arrest caries progression [20].
Compared with conventional SSC, the outcomes of the HT were found to be comparable to those of CT with preformed metal crowns. Regardless of whether complete, selective or no carious tissue removal was performed, the included studies consistently demonstrated high success rates for treatments involving SSCs over the years [9,14,15]. The effectiveness of both treatments has been attributed to the complete isolation of the tooth from the oral biofilm, which arrests caries progression by altering the biofilm beneath the crown [7]. Published literature has reported significant changes in the microbiota environment beneath dental restorations. These changes include not only a reduction in microbial load but also a decrease in microbial diversity within the infected dentine, along with genetic modifications to the biofilm [22].
Although both techniques showed similar outcomes, HT had several advantages over CT. CT was associated with higher levels of anxiety in children both before and after treatment, largely due to the use of local anaesthetics and the noise generated by high-speed handpieces. Another key advantage of the HT was the significantly reduced procedure time. On average, CT required approximately 40 minutes, whereas the HT took only 9 minutes, making it far more convenient for both practitioners and patients. Additionally, the HT was considered the most suitable treatment option in resource-limited environments, even in the absence of electricity or a dental chair [9,14,23,24]. However, an in vitro study comparing marginal fit and microleakage between conventional SSCs and Hall SSCs reported that the HT demonstrated significantly greater microleakage than CT with SSCs [25]. When comparing HT with traditional restorative materials, results consistently showed that the HT achieved superior outcomes. Significantly higher survival rates were recorded for the HT compared to conventional CT using various materials, including compomer, composite resin, glass ionomer, and amalgam [13,15]. Consequently, the use of SSCs is recommended for multi-surface caries due to the advantages of full-coverage restoration and superior durability [15]. While some variability was reported in survival rates for different restorative materials, no conflicting findings emerged regarding the effectiveness and durability of SSCs. Despite the high survival rate and simplicity of the HT, a minimum level of training is required to perform the technique. Additionally, SSCs have very limited aesthetic appeal, making them unsuitable for children and parents with aesthetic concerns [26]. In certain cases, two treatment sessions may be necessary, such as when orthodontic separators are required to open tight contacts [26]. As a result, careful case selection is essential before recommending the HT. There is no single perfect restoration for every case. The decision should consider not only the tooth but also the broader context, including the child, the parent’s preferences, and the clinician’s expertise [27-28].
Conclusion
This review revealed that the HT presented high performance in treating primary molars with moderate carious lesions with vital pulp. However, the success of this technique heavily depends on an accurate diagnosis of pulp status.
Recommendations
At the conclusion of this review, some recommendations were proposed:
While precise manipulation of the HT is important, adhering to its indications and ensuring an accurate diagnosis are crucial for its success
- HT should be the restoration of choice for proximal and multi-surface caries, particularly in children at high risk of developing new caries. This is due to the high efficiency and longevity provided by the full coverage of SSCs.
- ART and CT should be considered over HT for Class II restoration if the tooth is nearly exfoliated.
- CT treatment should be considered over HT for cooperative patients, Class I and II restorations with low to moderate risk and when esthetics are required by the patient or parent. However, the use of conventional GIC should be abandoned for Class II restorations as it showed low performances [27,28].
- HT is an excellent alternative for treating uncooperative or very young children where moisture control is challenging.
- HT offers excellent survival rates and should be prioritised in deprived communities where materials or functional equipment are limited. Its cost-effectiveness compared to CT, in terms of materials, durability, and time, makes it highly beneficial [14,19].
- HT should be considered to minimise infection dissemination during pandemic periods, as it is a non-aerosol generating procedure (non-AGP).
- Further education on the placement of preformed metal crowns using the HT is required for students and young practitioners.
- NRCT should be indicated for moderate to deep carious lesions or with hardly restorable teeth with near exfoliation date. This is particularly relevant in cases where restorative materials are unavailable or unaffordable. Successful treatment requires high levels of motivation and parental involvement in maintaining good oral hygiene practices.
Conflicts of interest
The author declares no conflict of interest.
References
- Ajai S, Mahalakshmi K (2021) Minimally invasive dentistry–A review. Intl J Community Dent 9: 97.
- Gunda S, Varma N (2013) Minimal intervention in pediatric dentistry. J Orofac Res 3: 28-33.
- Sharma P, Dhawan P, Rajpal S, Bhagat N (2021) Minimal invasive dentistry: An emerging trend. Int J Med Diagn Res 5: 34-41.
- Murali R (2017) Minimal invasive techniques in pedodontics-A Review. J Pharma Sci Res 9: 483.
- Evans DJ, Southwick CA, Foley JI, Innes NP, Pavitt SH (2000) The hall technique: A pilot trial of a novel use of preformed metal crowns for managing carious primary teeth. Citation: Tuith Online.
- Welbury RR (2017) The hall technique 10 years on: Its effect and influence. Br Dent J 222: 421-422. [Crossref]
- Innes N, Stewart M, Souster G, Evans D (2015) The hall technique; retrospective case-note follow-up of 5-year RCT. Br Dent J 219: 395-400. [Crossref]
- Narbutaite J, Santamaría RM, Innes N, Splieth CH, Maciulskiene V (2024) Comparison of three management approaches for dental caries in primary molars: A two-year randomized clinical trial. J Dent 150: 105390. [Crossref]
- Ayedun OS, Oredugba FA, Sote EO (2021) Comparison of the treatment outcomes of the conventional stainless steel crown restorations and the hall technique in the treatment of carious primary molars. Niger J Clin Pract 24: 584-594. [Crossref]
- Boyd DH, Thomson WM, Leon de La Barra S, Fuge KN, Van den Heever R, et al. (2021) A primary care randomized controlled trial of hall and conventional restorative techniques. JDR Clin Trans Res 6: 205-212. [Crossref]
- Araujo MP, Uribe S, Robertson MD, Mendes FM, Raggio DP, et al. (2020) The hall technique and exfoliation of primary teeth: A retrospective cohort study. Br Dent J 228: 213-217. [Crossref]
- Ebrahimi M, Shirazi AS, Afshari E (2020) Success and behavior during atraumatic restorative treatment, the Hall technique, and the stainless steel crown technique for primary molar teeth. Pediatr Dent 42: 187-192. [Crossref]
- Santamaría RM, Innes NP, Machiulskiene V, Schmoeckel J, Alkilzy M, et al. (2018) Alternative caries management options for primary molars: 2.5-year outcomes of a randomised clinical trial. Caries Res 51: 605-614. [Crossref]
- Elamin F, Abdelazeem N, Salah I, Mirghani Y, Wong F (2019) A randomized clinical trial comparing hall vs conventional technique in placing preformed metal crowns from Sudan. PLoS One14: e0217740. [Crossref]
- Kaptan A, Korkmaz E (2021) Evaluation of success of stainless steel crowns placed using the hall technique in children with high caries risk: A randomized clinical trial. Niger J Clin Pract 24: 425-434. [Crossref]
- Pascareli-Carlos AM, Tedesco TK, Calvo AF, Floriano I, Gimenez T, et al. (2023) Survival rate of the Hall technique compared with resin composite restoration in multi-surface cavities in primary teeth: A 1-year randomized clinical trial. J Appl Oral Sci 31: e20230048. [Crossref]
- Gugnani N, Pandit IK, Srivastava N, Gupta M, Sharma M (2010) International caries detection and assessment system (ICDAS): A new concept. Int J Clin Pediatr Dent 4: 93-100. [Crossref]
- Kassa D, Day P, High A, Duggal M (2009) Histological comparison of pulpal inflammation in primary teeth with occlusal or proximal caries. Int J Paediatr Dent 19: 26-33. [Crossref]
- Schwendicke F, Frencken J, Innes N (2018) Clinical recommendations on carious tissue removal in cavitated lesions. Monogr Oral Sci 27: 162-166. [Crossref]
- Amend S, Seremidi K, Kloukos D, Bekes K, Frankenberger R, et al. (2022) Clinical effectiveness of restorative materials for the restoration of carious primary teeth: An umbrella review. J Clin Med 11: 3490. [Crossref]
- Schwendicke F (2017) Contemporary concepts in carious tissue removal: A review. J Esthet Restor Dent 29: 403-408. [Crossref]
- Paddick JS, Brailsford SR, Kidd EA, Beighton D (2005) Phenotypic and genotypic selection of microbiota surviving under dental restorations. Appl Environ Microbiol 71: 2467-2472. [Crossref]
- Bhatia HP, Khari PM, Sood S, Sharma N, Singh A (2019) Evaluation of clinical effectiveness and patient acceptance of Hall technique for managing carious primary molars: An in vivo study. Int J Clin Pediatr Dent 12: 548-552. [Crossref]
- Alamoudi RA, Basudan S, Mahboub M, Baghlaf K (2022) Impact of COVID-19 pandemic on dental treatment in children: A retrospective cross-sectional analysis in Jeddah City. Clin Cosmet Investig Dent 13: 95-102. [Crossref]
- Erdemci ZY, Cehreli SB, Tirali RE (2014) Hall versus conventional stainless steel crown techniques: In vitro investigation of marginal fit and microleakage using three different luting agents. Pediatr Dent 36: 286-290. [Crossref]
- Innes N, Evans D, Hall N (2009) The hall technique for managing carious primary molars. Dent Update 36: 472-478. [Crossref]
- Chisini LA, Collares K, Cademartori MG, de Oliveira LJ, Conde MC, et al. (2018) Restorations in primary teeth: A systematic review on survival and reasons for failures. Int J Paediatr Dent 28: 123-139. [Crossref]
- Smales RJ, Yip HK (2000) The atraumatic restorative treatment (ART) approach for primary teeth: Review of literature. Pediatr Dent 22: 294-298. [Crossref]