We present a rare case of localised, biopsy proven vaginal melanoma and vaginal melanosis in a Caucasian 66 year old who presented with postmenopausal bleeding. A systematic literature review of journal articles published between December 2013 and November 2015 was performed for studies conducted in Europe and the United States of America using Medline and Pubmed. Articles were selected for review if they included large (over 10 cases) retrospective analysis, epidemiological review and genetic analysis of primary vaginal melanoma and/or primary vulvar melanoma. Our findings demonstrate the challenges of researching and treating rare diseases.
Introduction
Melanoma can arise from any mucosal epithelium lining including the vulvovaginal. It is more likely to be multifocal and carries a worse prognosis than cutaneous melanoma.Primary Vaginal melanomas are extremely rare with an estimated incidence of 0.026/100,000 women per year [1]. As a result there is limited understanding of the pathogenesis, risk factors and optimal treatments for primary vaginal melanoma.
Case
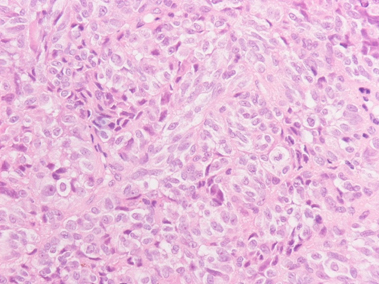
A 64 year old lady presented to her GP with a six week history of postmenopausal bleeding. Her background was significant for a hysterectomy in 2001 and bilateral salpingo-oophorectomy for endometriosis. She is a social smoker. She was referred to the gynaecology service and underwent an Examination under Anaesthesia (EUS) and cystoscopy which revealed a lesion at the right side of the vaginal vault approximately 2-3 cm in size, which was resected. There was a small amount of residual lesional tissue present. The vulva and urethra were normal. Pathology revealed an invasive malignant melanoma (Figure 1).
Figure 1. H&E, Original Magnification 400X. Vaginal Biopsy (first procedure). Multiple fragments of high grade malignant tumour with large areas of necrosis. Immunohistochemistry showed tumour cells to be MelanA, HMB45 and S100 positive as well as focally p53 positive. The findings are consistent with invasive malignant melanoma.
Her case was reviewed at the Gynaecological multidisciplinary meeting and she was subsequently admitted electively for a laparoscopic vaginectomy. However multiple foci of dark lesions were noted on the upper, mid posterior, left lateral and left anterior vaginal wall which were not amenable for complete excision with the planned procedure so only vaginal biopsies were taken revealing areas of vaginal melanosis and malignant melanoma in situ (Figure 2 and 3). PET CT revealed no evidence of distant disease. Her case was discussed at the Oncology MDM and the decision was made to proceed to vaginectomy with radiation if the surgical margins were positive.
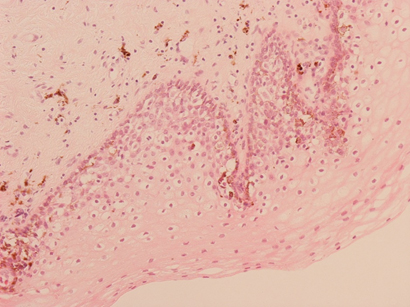
Figure 2. H&E, Original Magnification 200X. Left anterior vagina (second procedure). Large atypical melanocytes with clear cytoplasm with mitoses are present in the lower third of the epithelium, with no invasive component identified. Subepithelial melanophages are also present. The findings are consistent with malignant melanoma in situ. Immunohistochemistry (MelanA and HMB45) was supportive of this diagnosis.
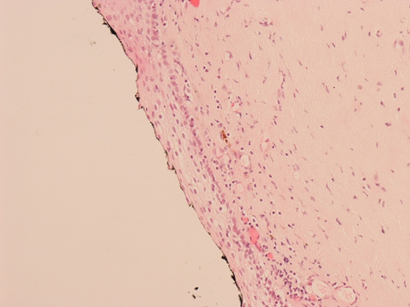
Figure 3. H&E, Original Magnification 200X. Posterior vagina (second procedure). Increased subepithelial melanophages as well as subepithelial chronic inflammation is present. There are no atypical melanocytes present. The findings are consistent with vaginal melanosis. Immunohistochemistry (MelanA and HMB45) was supportive of this diagnosis. Note that a small amount of black surface marking ink is present.
Discussion
Vaginal melanoma has five-year survival rates of between 5-20% [2]. The aetiology is poorly understood .Several risk factors have been implicated, including; chronic inflammatory disease, viral infections and chemical irritants [3]. The majority of patients will develop metastatic disease regardless of treatment intervention. Several different modalities have been used; extensive surgical resection versus conservative excision and radiation [4]. It is unclear if there is any additional survival gain from lymphadenectomy [5,6]. In the metastatic setting primary vaginal melanoma has limited response to cytotoxic regimens. Platinum /taxanes have been used with response rates up to 20% [7]. Ipilimumab and vemurafenib are approved for use despite the fact that there were no trials in this setting as data was extrapolated from trials done in cutaneous melanoma [7].
Microscopically, most vaginal malignant melanomas contain sheets of cells which vary from bland to very irregular and are not indicative of any common type of vaginal cancer [8]. Prognostic factors are debated (8), however a recent study showed mitotic count and lymph node status were the most important histological prognostic factors for disease free survival [9]. Mucosal melanosis, of which genital and specifically vaginal melanosis is a type, is a benign lesion which can mimic melanoma clinically [10-12]. They can however be differentiated histologically [13]. Mucosal melanosis is associated with the following features; increased pigmentation of basal keratinocytes, increased melanocytes without atypia and pigment incontinence into the subepithelium [11-16]. The combination of both vaginal melanoma and vaginal melanosis in the same patient has been documented [17], however is exceptionally rare. It has been suggested that mucosal melanosis is a possible precursor of melanoma [17], however one recent long term follow up of patients with vulval melanosis revealed no progression of melanosis to melanoma [18]. Overall, genital, including vaginal, melanosis is considered benign and conservative management with follow up to monitor for progression and treating this accordingly if present is the current standard of treatment [18,19].
A systematic literature review of journal articles related to vaginal and/or vulvar melanoma published between December 2013 and November 2015 was performed for studies conducted in Europe and the United States of America (USA), using Medline and Pubmed. Articles were selected for review if they included large (over 10 cases) retrospective analysis, epidemiological review, and genetic analysis of primary vaginal melanoma and/or primary vulvar melanoma (Table 1).
Table 1. Literature Review of Case Series between of Primary Vaginal and Vulvar Melanoma 2013-2015
Reference
Study Type
Patient Population
Results
[7]
Case Series
15 vulvar melanoma
5 vaginal melanoma
Vulvar
BRAF mutation7.6%
C-KITmutation27.6%
NRAS mutation 27.6%
Vaginal
1 TP53 mutation 7
[20]
Retrospective analysis
14 vaginal melanoma
4 cervical melanomas
5 urethral melanomas
1 vulvar melanoma.
NRAS mutations (4/24, 21%)
KIT mutations (1/24, 4%),
BRAF mutations absent
3/4 NRAS mutations were in vaginal melanomas (21%)
mainly affecting codon 61
1 KIT mutation was in a vaginal melanoma effecting exon 17
[3]
Retrospective analysis
44 vaginal melanoma
median follow-up 18.9 months
68.2% recurrences
21 (47.7%) died of disease
Median PFS 14.4 months
median OS 39.5 month
Depth of invasion associated with OS (P = 0.023)
[4]
Case Series
31 vaginal melanoma
median age 58 years
22 surgery
7 chemotherapy
19 immunotherapy
median follow-up 20.2 months
5-year OS 32.3%.
[21]
Epidemiological Study
762 vulvar and vaginal melanoma
28 black patients
350 (45.9%) presented with localized disease (P < 0.0001)
median survival of black patients 16months
median survival in the nonblack population was 39 months
[5]
Retrospective analysis
24 primary vaginal melanoma
Treatment
42 surgery
9 local adjuvant treatment
10 systemic therapy
Median relapse-free survival was 10.9 months.
C-KIT-negative status (P=0.01) associated with locoregional recurrence.
Median overall survival (OS) was 28.4 months.
Involvement of lymph node metastasis decreased OS (P < 0.01).
[6]
See comment in PubMed Commons below[]
Case series
36 post surgery for primary vaginal melanoma
14 post surgery for vulvar melanoma
.
5-year OS rate was 30.9%, with median OS of 3.3 years.
Vulvar melanoma no improved OS (p = 0.39)
1 patient with vaginal melanoma had a partial response to carboplatin /paclitaxel .After further surgical resection and adjuvant carboplatin/paclitaexland bevacizumab is disease free at 5 years.
Six journals involving 953 patients, 336 had vaginal melanoma and 617 had vulvar melanomas. The median OS for vaginal melanoma was 39 months [2,4-6]. Two studies performed genetic analysis, which revealed; 1/15 vulvar melanomas had a BRAF mutation, 4/15 had a NRAS mutation and 3/14 had a C-KIT mutation. 3/14 vaginal melanomas had an NRAS mutation [7,20]. Median survival in patients who were black was significantly reduced; 16 months versus 39 months [9].
Our results confirm the poor outcomes of vaginal and vulvar melanomas despite multiple treatment options [21]. Genetic analysis revealed differences in targetable mutations between vulvar and vaginal melanoma. This suggests that they should be studied as separate entities, and treatments should be tailored accordingly. Further study is required to understand differences in outcomes between the different targetable mutations and between black and non-black patients.
In conclusion primary vaginal melanoma, especially in the setting of mucosal melanosis, demonstrates the challenges of researching and treating rare diseases. A proportion of these tumors will harbor an activating mutation and may respond to targeted agents. The role of immunotherapy requires further assessment. Overall a collaborative treatment making process should be undertaken with quality of life and patient preference being prioritised.
References
Weinstock MA (1994) Malignant melanoma of the vulva and vagina in the United States: patterns of incidence and population-based estimates of survival. Am J Obstet Gynecol 171: 1225-1230. [Crossref]
Wechter ME, Gruber 2021 Copyright OAT. All rights reservet al. (2004) Vulvar melanoma: a report of 20 cases and review of the literature. J Am Acad Dermatol 50: 554-562. [Crossref]
Xia L, Han D, Yang W, Li J, Chuang L, Wu X (2014) Primary malignant melanoma of the vagina: a retrospective clinicopathologic study of 44 cases. Int J Gynecol Cancer 24: 149-155. [Crossref]
Huang Q, Huang H, Wan T, Deng T, Liu J (2013) Clinical outcome of 31 patients with primary malignant melanoma of the vagina. J Gynecol Oncol 24: 330-335. [Crossref]
Vaysse C, Pautier P, Filleron T, Maisongrosse V (2013) A large retrospective multicenter study of vaginal melanomas: implications for new management. Melanoma Res 23: 138-146. [Crossref]
Markovic SN, Weaver AL, Cliby WA (2013) Vulvar and vaginal melanoma: case series and review of current management options including neoadjuvant chemotherapy. Gynecol Oncol 129: 533-537. [Crossref]
Rouzbahman M, Kamel-Reid S, Al Habeeb A, Butler M, Dodge J, et al. (2015) Malignant Melanoma of Vulva and Vagina: A Histomorphological Review and Mutation Analysis--A Single-Center Study. JLow Genit Tract Dis 19: 350-353. [Crossref]
Robboy SJ, Mutter GL, Prat J, Bentley RC, Russell P, et al. (2008) Robboy’s Pathology of the Female Reproductive Tract (2nd edn). London: Churchill Livingstone.
Ditto A, Bogani G, Martinelli F, Di Donato V, Laufer J, et al. (2016) Surgical Management and Prognostic Factors of Vulvovaginal Melanoma. J Low Genit Tract Dis 20: e24-29. [Crossref]
Crowson AN, Magro CM, Mihm Jr MC (2001) The Melanocytic Proliferations: A Comprehensive Textbook of Pigmented Lesions. New Jersey: Wiley-Blackwell.
Karney MY, Cassidy MS, Zahn CM, Snyder RR (2001) Melanosis of the vagina. A case report. JReprod Med 46: 389-391. [Crossref]
Tsukada Y (1976) Benign melanosis of the vagina and cervix. Am J Obstet Gynecol 124: 211-212. [Crossref]
Lee BS, Yoon TJ, Oh CW, Kim TH (1996) A Case of Vulvar Melanosis. Ann Dermatol 8: 275.
Mannone F, De Giorgi V, Cattaneo A, Massi D, De Magnis A, et al. (2004) Dermoscopic features of mucosal melanosis. Dermatol Surg 30: 1118-1123. [Crossref]
Estrada R, Kaufman R (1993) Benign vulvar melanosis. J Reprod Med 38: 5-8. [Crossref]
Sison-Torre EQ, Ackerman AB (1985) Melanosis of the vulva. A clinical simulator of malignant melanoma. Am J Dermatopathol 7: 51-60. [Crossref]
Lee RB, Buttoni L Jr, Dhru K, Tamimi H (1984) Malignant melanoma of the vagina: a case report of progression from preexisting melanosis. Gynecol Oncol 19: 238-245. [Crossref]
Jones I (2012) Melanosis of the vulva: A long-term follow-up from Brisbane, Australia. Open Journalof Obstetrics and Gynaecology 2: 247-249.
Núñez-Troconis J, Delgado M, González G, Rivas A, Molero K (2011) Melanosis of the vagina and human papillomavirus infection, an uncommon pathology: case report. Invest Clin 52: 268-273. [Crossref]
van Engen-van Grunsven AC, Küsters-Vandevelde HV, De Hullu J, et al. (2014) NRAS mutations are more prevalent than KIT mutations in melanoma of the female urogenital tract--a study of 24 cases from the Netherlands. Gynecol Oncol 134: 10-14. [Crossref]
Mert I, Semaan A, Winer I, Morris RT, Ali-Fehmi R (2013) Vulvar/vaginal melanoma: an updated surveillance epidemiology and end results database review, comparison with cutaneous melanoma and significance of racial disparities. Int J Gynecol Cancer 23: 1118-1125. [Crossref]
Editorial Information
Editor-in-Chief
Masayoshi Yamaguchi
Emory University School of Medicine
Article Type
Case Report
Publication history
Received: April 15, 2016
Accepted: May 03, 2016
Published: May 07, 2016
Kelly D, Gleeson J, Watson G, Woods G, O’Keane C, et al. (2016) Primary vaginal melanoma in the setting of acquired mucosal melanosis - A case report and literature review. Integr Cancer Sci Therap. 3: DOI: 10.15761/ICST.1000190.
Corresponding author
Deirdre Kelly
Departments of Medical Oncology, Mater Misericordiae University Hospital, Eccles St., Dublin 7, Ireland, Tel: 0860706237.
Table 1. Literature Review of Case Series between of Primary Vaginal and Vulvar Melanoma 2013-2015
Reference
Study Type
Patient Population
Results
[7]
Case Series
15 vulvar melanoma
5 vaginal melanoma
Vulvar
BRAF mutation7.6%
C-KITmutation27.6%
NRAS mutation 27.6%
Vaginal
1 TP53 mutation 7
[20]
Retrospective analysis
14 vaginal melanoma
4 cervical melanomas
5 urethral melanomas
1 vulvar melanoma.
NRAS mutations (4/24, 21%)
KIT mutations (1/24, 4%),
BRAF mutations absent
3/4 NRAS mutations were in vaginal melanomas (21%)
mainly affecting codon 61
1 KIT mutation was in a vaginal melanoma effecting exon 17
[3]
Retrospective analysis
44 vaginal melanoma
median follow-up 18.9 months
68.2% recurrences
21 (47.7%) died of disease
Median PFS 14.4 months
median OS 39.5 month
Depth of invasion associated with OS (P = 0.023)
[4]
Case Series
31 vaginal melanoma
median age 58 years
22 surgery
7 chemotherapy
19 immunotherapy
median follow-up 20.2 months
5-year OS 32.3%.
[21]
Epidemiological Study
762 vulvar and vaginal melanoma
28 black patients
350 (45.9%) presented with localized disease (P < 0.0001)
median survival of black patients 16months
median survival in the nonblack population was 39 months
[5]
Retrospective analysis
24 primary vaginal melanoma
Treatment
42 surgery
9 local adjuvant treatment
10 systemic therapy
Median relapse-free survival was 10.9 months.
C-KIT-negative status (P=0.01) associated with locoregional recurrence.
Median overall survival (OS) was 28.4 months.
Involvement of lymph node metastasis decreased OS (P < 0.01).
[6]
See comment in PubMed Commons below[]
Case series
36 post surgery for primary vaginal melanoma
14 post surgery for vulvar melanoma
.
5-year OS rate was 30.9%, with median OS of 3.3 years.
Vulvar melanoma no improved OS (p = 0.39)
1 patient with vaginal melanoma had a partial response to carboplatin /paclitaxel .After further surgical resection and adjuvant carboplatin/paclitaexland bevacizumab is disease free at 5 years.
Figure 1. H&E, Original Magnification 400X. Vaginal Biopsy (first procedure). Multiple fragments of high grade malignant tumour with large areas of necrosis. Immunohistochemistry showed tumour cells to be MelanA, HMB45 and S100 positive as well as focally p53 positive. The findings are consistent with invasive malignant melanoma.
Figure 2. H&E, Original Magnification 200X. Left anterior vagina (second procedure). Large atypical melanocytes with clear cytoplasm with mitoses are present in the lower third of the epithelium, with no invasive component identified. Subepithelial melanophages are also present. The findings are consistent with malignant melanoma in situ. Immunohistochemistry (MelanA and HMB45) was supportive of this diagnosis.
Figure 3. H&E, Original Magnification 200X. Posterior vagina (second procedure). Increased subepithelial melanophages as well as subepithelial chronic inflammation is present. There are no atypical melanocytes present. The findings are consistent with vaginal melanosis. Immunohistochemistry (MelanA and HMB45) was supportive of this diagnosis. Note that a small amount of black surface marking ink is present.