Abstract
Health literacy was first introduced in the 1970s in the United States and Canada, and its initial focus was limited solely to the ability to understand health information related to healthcare. With the advent of the internet and the information explosion phenomenon in the early 1980s, this concept expanded based on the foundations of "information literacy," and a fundamental paradigm shift occurred. In the contemporary view, health literacy is strongly linked to basic literacy and includes individuals' knowledge, competence, and motivation for a four-stage process: Access (finding and obtaining information), Understanding (comprehending information), Evaluation (interpreting and judging information), and Application (practical use of information). Each of these stages represents a fundamental dimension of health literacy, which depends both on individual characteristics and the quality of the information, and encompasses the three levels: functional, interactive, and critical. The level and need for health literacy in a society are highly dependent on the basic medical literacy of its individuals, which in turn is influenced by the type of healthcare system and the health insurance structure of that country. For example, in a country like the United Kingdom with a universal insurance system and free healthcare, people generally enjoy a higher level of health literacy. Another crucially important determining factor is the level of maturity of information and communication technology in a society. In communities that are at a rudimentary level in terms of using information technologies, the understanding of health literacy remains limited to the 1970s definition, namely the promotion of basic medical literacy. This concept has two dimensions: individual and organizational; the organizational dimension is the responsibility of organizations to help people find and use health information and services by becoming health-centric institutions. Finally, with the increasing growth in the use of information and communication technology in societies, the concept of health literacy has evolved from "e-health literacy" towards "digital health literacy," indicating the complete penetration of the digital environment into all dimensions of the health system.
Keywords
health literacy, electronic health literacy, digital health literacy, individual health literacy, organizational health literacy
Introduction
The historical and conceptual framework of health literacy
Although the concept of health literacy is semantically related to the concept of information literacy, it cannot reflect its content as effectively in comparison. Information literacy means the ability to deal with a large volume of information in such a way that one can search, evaluate, select, and use quality information from reliable sources. Health literacy is defined as the ability to obtain, read, understand, and use healthcare information to make appropriate health decisions and follow treatment instructions [1]. However, upon initially hearing or encountering this term, an incorrect perception often forms in the audience's mind. It seems the reason for this misinterpretation is that the word "literacy" combined with the word "health" suggests a concept implying the transmission of health knowledge. There are numerous definitions of health literacy [2]. Part of this issue stems from the fact that health literacy depends on the context or situation in which its demands arise (for example: healthcare, media, the internet, or sports centers) and also on the skills that individuals bring to that situation [3].
Health literacy first emerged in the 1970s in the United States and Canada, before the information explosion phenomenon and the advent of the concept of information literacy. Its initial focus was on the ability to understand health information related to healthcare. It is noteworthy that since then, it has evolved as a concept and field of research globally [4]. With the emergence of the internet and the information explosion in the early 1980s, this focus expanded based on the concept of information literacy, and a paradigm shift occurred. Today, health literacy generally focuses on a set of skills and competencies required for accessing, understanding, evaluating, and applying health information in the domains of healthcare, disease prevention, and health promotion [5]. In the 1998 Health Promotion Glossary, the World Health Organization (WHO) defines health literacy as: "The cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand, and use information in ways which promote and maintain good health. Health literacy implies the achievement of a level of knowledge, personal skills, and confidence to take action to improve personal and community health by changing personal lifestyles and living conditions. Thus, health literacy means more than being able to read pamphlets and make appointments. With the emergence of the internet and the availability of health websites, which have improved people's access to health information and their growing ability to use it effectively, health literacy is crucial for empowering all members of the community [6]. The level or degree of basic or general medical literacy in a society determines the need for health literacy, and this itself can depend on the type of healthcare system and the type of health insurance. For example, in England, where healthcare is free due to the universal insurance coverage in the country, people enjoy a high level of health literacy. Whereas in the United States, because health insurance coverage is not universal and healthcare involves costs, the level or degree of public health literacy is not as high as in England.
Another very important factor that reflects a meaning of health literacy beyond the understanding that existed before the 1980s – which was basic medical literacy appropriate to the state of the community's health system – is the potential for applying information technology and its growing use in society. If a society is in a very primitive condition regarding the use of information and communication technology (like some Asian and African countries), then it is evident that its people's perception of health literacy would be the same as it was in the 1970s in Western countries: namely, the promotion and transmission of basic medical literacy in society.
This diversity in the perception of the concept of health literacy around the world has led experts like Don Nutbeam to propose a definition with a broader semantic range than what is typically associated with the concept of health. In the year 2000, Nutbeam operationalized the World Health Organization's definition of health literacy and presented a conceptual model with three levels: Basic/Functional health literacy, Communicative/Interactive health literacy, and Critical health literacy. What was initially defined as having sufficient skills in reading and writing and basic health awareness (Basic/Functional health literacy) gradually evolved into a competency for performing knowledge-based, literacy-oriented tasks aimed at greater control over life events and situations (Critical health literacy). Higher levels of health literacy also lead to greater autonomy and personal empowerment [7].
During the final review of the World Health Organization report, it became clear that the organization had updated its 1998 Health Promotion Glossary and revised the definition of health literacy. In the new glossary of health promotion terminology, health literacy is defined as: "The personal knowledge and competencies which are accumulated through daily activities, social interactions, and across generations. Personal knowledge and competencies are shaped by organizational structures and access to resources that enable individuals to access, understand, evaluate, and use information and services in ways that promote and maintain the health and well-being of themselves and those around them" [8].
In 2012, Sorensen and colleagues, et al. [9] published a systematic review of existing definitions and concepts of health literacy in the international literature. This systematic review led to several definitions and conceptual models of health literacy, which guided a content analysis and ultimately resulted in the creation of an integrated model of health literacy (Figure 1). This model shows the main dimensions of health literacy (depicted in the concentric ovals in the center of the figure), along with a logical model explaining both proximal and distal factors influencing health literacy, as well as the pathway linking health literacy to health outcomes [9].
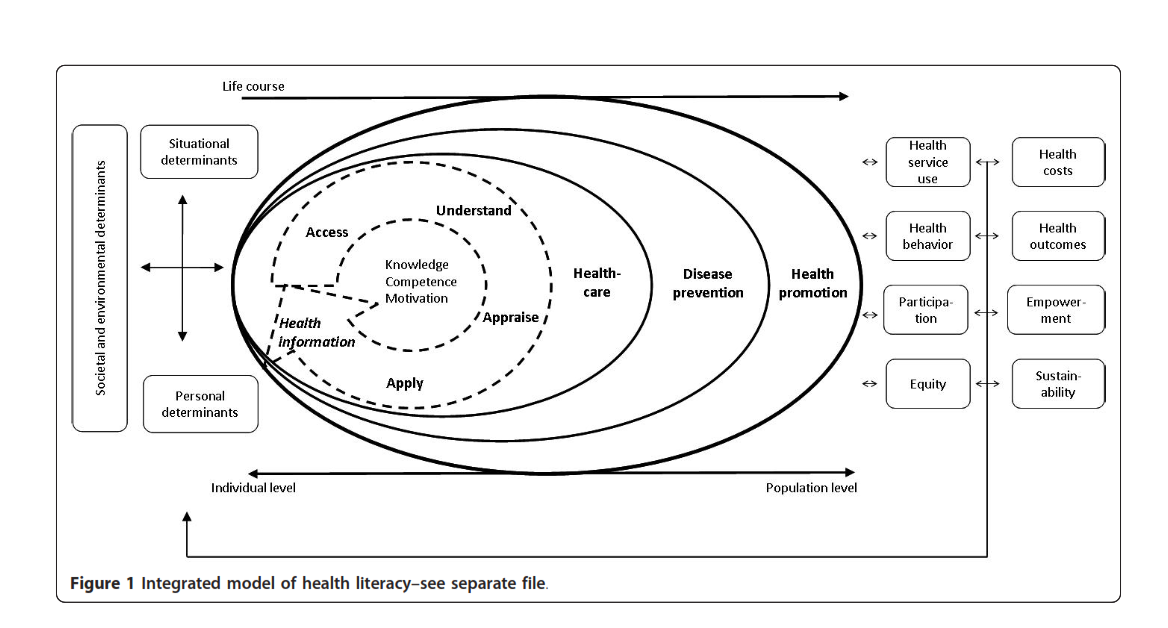
Figure 1. Integrated model of health literacy
Health literacy is strongly linked to basic literacy and includes individuals' knowledge, competencies, and motivation to access (find, seek, and obtain health information), understand (comprehend the obtained health information), appraise (interpret, judge, and evaluate health information), and apply (communicate and use health information). Each step in this process represents a fundamental dimension of health literacy, which depends both on the individual's cognitive and psychosocial characteristics and on the quality of the provided information. This process also encompasses the functional, interactive, and critical levels of health literacy defined by Nutbeam (2000) [5].
The process of accessing, understanding, appraising, and applying health information develops skills and competencies that enable an individual to make decisions and judgments in daily life across three healthcare domains: disease prevention, health promotion, and healthcare. However, since contextual demands change over time and the ability to navigate the health system depends on cognitive and psychosocial development, as well as past and present experiences, health literacy competencies and skills develop throughout life and are linked to lifelong learning. Health literacy is also influenced by factors such as social and environmental determinants (e.g., demographics, culture, language, political forces, social structures), individual factors (age, gender, race, socioeconomic status, education, occupation, income, literacy level), and situational factors (social support, family and peer influence, media use, physical environment).
Health literacy can influence health behaviors and the use of health services, thereby altering health outcomes and healthcare costs. Promoting health literacy gradually increases personal autonomy and empowerment, and the process of health literacy can be considered part of personal development for improving quality of life. At the population level, this promotion can lead to greater equity and sustainability in public health changes. "Limited health literacy" can be compensated for both by educating individuals to become more empowered (promoting individual health literacy) and by simplifying tasks and conditions (such as improving the readability of the health system and the information provided) [9]. Today, the integrated model by Sørensen, et al. [9] is widely used in international literature and research to explain the concept of health literacy.
Potential intervening factors in the health literacy framework
Figure 2 shows three key sectors that should take responsibility for health literacy and within which health literacy skills can be enhanced. These sectors, which constitute the contexts for health literacy, include culture and society, the health system, and the education system. These sectors also provide intervention points that represent both challenges and opportunities for improving health literacy.

Figure 2. Illustrates the interaction of individuals with education systems, health systems, and social factors in relation to health literacy
Figure 2 illustrates the interaction of individuals with education systems, health systems, and social factors in relation to health literacy. This figure is not a causal model. The determinants of health literacy are likely as complex and diverse as the most complex current problems in the health domain. Although causal relationships between "limited health literacy" and health outcomes have not yet been definitively proven, cumulative and consistent findings suggest such a link exists. More research is needed to determine the nature of these causal relationships among these factors. Mapping this causal network should be a goal for research, but it is important to note that current knowledge can form a basis for changes in practice and policy.
In the following, the role of each of these sectors in supporting or undermining health literacy is introduced.
Culture and society
Culture is defined as the shared ideas and values people learn from society, which shape their beliefs and how they interact with the healthcare system. Factors like language, income, and media, known as the social determinants of health, also affect a person's health literacy. Since culture is essential for understanding human experience and American culture is shaped by various historical and social forces, these cultural contexts must be used to achieve a health-literate society in America.
The education system
The education system in the United States, encompassing K-12, adult education, and higher education, is fundamental for developing literacy and skills. The K-12 system builds a foundation in English and numeracy, progressing to more complex comprehension. Adult education serves those who did not complete or succeed in K-12, older adults, and immigrants seeking education or English language skills. This report primarily focuses on these groups, as individuals with college degrees typically have adequate literacy. The education of health professionals is also included within this framework.
The health system
The healthcare system involves designing health messages, shaping policies, conducting research, and enforcing regulations. This term includes all staff in hospitals, clinics, public health organizations, and insurance companies. Scientific literature and the committee's research consistently show that an individual's health literacy affects how they interact with the healthcare system and can influence their health status and outcomes [10].
Health literacy includes both personal and organizational health literacy. Personal health literacy relates to how well an individual can find and understand the health information and services they need. It also refers to the ability to use this information and these services to make correct decisions about health. Organizational health literacy relates to how well organizations help individuals find the health information and services they need. It also includes helping people use this information to make correct health decisions [11]. Accordingly, the Australian Commission on Safety and Quality divides health literacy into two parts: personal and environmental. Personal health literacy: the skills, knowledge, motivation, and capacity of an individual to access information, understand, evaluate, and apply it for effective decision-making about health and healthcare, and to take appropriate actions. The health literacy environment: the infrastructure, policies, processes, materials, people, and relationships that constitute the healthcare system and influence how health-related information and services are accessed, understood, evaluated, and applied [12].
Organizational health literacy
Although health literacy has often been defined and introduced as an individual characteristic, there is growing recognition that health literacy does not depend solely on individual skills. Rather, it is the product of the interaction between individuals' abilities and the demands and complexities of the healthcare system. To better align the demands of the healthcare system with people's skills and abilities, systemic and organizational changes are needed [13]. A health-literate organization can be described as follows: an organization that helps people find, understand, and use information and services to care for their health [14]. There are various options for becoming a health-literate organization, and healthcare organizations can choose different strategies. What matters is how effective these strategies are for the different population groups that the organization serves [15].
Brach and colleagues (2012) introduced a list of 10 attributes of a health-literate organization. This list is not exhaustive and may not be applicable to all communities, but it represents an effort to synthesize existing knowledge and experience supported by health literacy research. Organizations possessing these attributes create an environment where individuals can optimally benefit from healthcare services. These attributes are:
1. Has leadership that considers health literacy an integral part of its mission, structure, and operations.
2. Integrates health literacy into planning, evaluation, patient safety, and quality improvement.
3. Prepares the workforce to be health literate and monitors progress.
4. Involves the population it serves in the design, implementation, and evaluation of health information and services.
5. Meets the needs of populations with varying levels of health literacy and avoids labeling.
6. Uses health literacy strategies in interpersonal communications and confirms understanding in all contacts.
7. Provides easy access to health information and services and assistance with navigation.
8. Designs and distributes print, audiovisual, and social media content that is understandable and actionable.
9. Addresses health literacy in high-risk situations, such as care transitions and communications about medications.
10. Clearly explains health insurance coverage and costs that individuals are responsible for paying.
These attributes relate to the structure and operations within the organization, the design and delivery of information, communications, and services, as well as the knowledge of the organization's staff. They also demonstrate that health organizations can take immediate, concrete, and tangible actions to bridge the gap between individuals' health literacy skills and the complex demands of the healthcare system. Even if healthcare organizations invest in these attributes to a limited extent, it will still create an environment that improves people's access to and benefit from health services and will contribute to population health promotion [13].
Various factors can influence an individual's health literacy, including:
• The individual's knowledge of medical terms
• Understanding how the healthcare system functions
• The ability to communicate with healthcare providers
• The ability to find health information, which, depending on the level of information technology adoption in the society, may require computer skills
• Reading, writing, and numeracy skills
• Individual factors such as age, income, education, language abilities, and culture
• Physical or cognitive limitations
Many individuals at risk of "limited health literacy" also face health disparities. Health disparities refer to differences in health outcomes between different groups of people. These groups may be defined by age, race, gender, or other factors (Figure 3).

Figure 3. Shows the relationship between health literacy and the concepts of e-health literacy and digital health literacy
As previously mentioned, the concept of health literacy is deeply tied to the concept of information literacy. From the mid-1980s, as societies in both the East and West became dependent on the internet and computer-based information systems, along with the growth in the application of information and communication technology (ICT), health literacy began its semantic evolutionary path towards e-health literacy, which denotes specific characteristics, and then towards digital health literacy, indicating the digitization of the health system's environment. In any case, health literacy is an overarching concept and can also be introduced in electronic or digital forms. Understanding the distinction between an electronic health system and a digital one depends on knowledge of the evolutionary path of ICT use in countries worldwide.
The evolutionary progression of information and communication technology (ICT) and its application in the health sector began in the mid-1950s under the title "ICT in Health." A prominent feature of this period was the lack of a full societal understanding of ICT's application in the health system, and health information systems were sporadically and limitedly present in society. By the mid-1960s, with the specialized use of information and communication technology in the health field, we entered a period called "Health ICT." Characteristics of this period include the management-centric nature of community health information systems and the absence of a national plan for using this type of technology in the health system.
After three decades of growth and development of ICT and its application in the health sector, the concept of "e-Health" marked the beginning of a new era starting from the early 2000s, which remains relevant and common in many countries today. Characteristics of the e-Health stage include society having a full and comprehensive understanding of the application of information technology in the health system, and thus having an e-Health plan to achieve specific goals. Furthermore, all health information systems are patient-centric and operate within a national network.
The success of the Human Genome Project in 2003, announced by the NIH, paved the way for the emergence of a new branch of medicine called Personalized/Precision Medicine. Coupled with significant advancements in artificial intelligence in the fields of machine learning and robotics, along with the tremendous development of information technology in sensors and smartphones in 2015, and the emergence of nanotechnology, especially in electronics, these factors set the stage for the rise of an important phenomenon known as "Digital Health." This is recognized as the fourth period of ICT application in the health sector, with its birth estimated around the mid-2020s [16].
Conclusion
Health literacy is a dynamic and evolving concept that has developed from an initial focus on understanding health information into a four-stage process including access, understanding, evaluation, and application of information. This transformation has occurred under the influence of the information explosion and the emergence of the internet. The level of health literacy in any society primarily depends on basic medical literacy, which itself is influenced by the healthcare system and health insurance structure. Furthermore, the level of information technology maturity in a society plays a decisive role in understanding and implementing this concept, to the extent that in societies with advanced technology, health literacy is moving towards digital concepts. Ultimately, the full realization of health literacy requires simultaneous attention to both its individual and organizational dimensions.
Conflicts of interest
The author declares no conflict of interest.
Author contributions
The article was entirely prepared by Hamid Maghaddasi.
References
- Roundtable on Health Literacy; Board on Population Health and Public Health Practice; Institute of the Medicine (2012) Facilitating state health exchange communication through the use of health literate practices: Workshop summary. National Academies Press. ISBN 978-0-309-22029-3. International Osteoporosis Foundation (2024) Epidemiology of osteoporosis and fragility fractures | International Osteoporosis Foundation. www.osteoporosis.foundation
- Pleasant A, McKinney J (2011) Coming to consensus on health literacy measurement: An online discussion and consensus-gauging process. Nurs Outlook 59: 95-106. [Crossref]
- Atkinson, Richard C, Jackson, Gregg B (1992) Research and Education Reform.
- Simonds SK (1974) Health education as social policy. Health Education Monographs 2: 1-10.
- Nordens välfärdscenter. Health-literacy-concept-and-definition
- WHO (1998) Health promotion glossary.
- Nutbeam D (2000) Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot Int 15: 259-267.
- WHO (2021) Health promotion glossary.
- Sørensen K, Van den Broucke S, Fullam J, Doyle G, Pelikan J, et al. (2012) Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 12: 80. [Crossref]
- Institute of Medicine (US) Committee on Health Literacy, Nielsen-Bohlman L, Panzer AM, Kindig DA (2004) Health Literacy: A prescription to end confusion. Washington (DC): National Academies Press (US). [Crossref]
- NCBI. Medlineplus. Health Literacy. https://medlineplus.gov/healthliteracy.html
- Australian Commission on Safety and Quality in Health Care. National statement on health literacy. Sydney: ACSQHC; 2014.
- Brach C, Dreyer B, Schyve P, Hernandez LM, Baur C, et al. (2012) Attributes of a health literate organization. Inst Med 10.
- Farmanova E, Bonneville L, Bouchard L (2018) Organizational health literacy: Review of theories, frameworks, guides, and implementation issues. Inquiry 55: 0046958018757848. [Crossref]
- Kickbusch I, Pelikan JM, Apfel F, Tsouros A (2013) Health literacy. WHO Regional Office for Europe.
- Rowlands D (2019) What is digital health? And why does it matter. Health Informatics Society of Australia 2: 2023-2032.