Improving the functional mapping quality means overcoming the effect of boundary conditions affecting its sensitivity under the false negative impact without forgetting the manageable impact of false positives on its specificity. This is a simulation study of the functional brain mapping has been done by neuronal computational modeling in correlation with a comparative retrospective analysis. However, the results show the optimization of the parameters threshold in DES, as intensity threshold, its increase by the CSF resistivity and the extremum duration of the electrical signal in direct application. Therefore, the awake surgery becomes not only a revolutionary technique; because of the extent of the resection, which is currently done according to functional imperative, unlike the onco-anatomical limits during the classical paradigm; but to free up new therapeutic perspective towards a functional, personalized and maximalist surgical neuro-oncology without malignant transformation.
functional brain mapping, awake surgery, DES, stimulation threshold optimizing
Surgery in an awake condition after functional brain mapping by direct electrical stimulation DES remains a revolutionary technique due to the extent of resection, which is currently done according to functional imperative, unlike the onco-anatomical limits during the classical paradigm. Indeed, the total functional recovery of deficits expresses the effectiveness and efficiency of this specific technique, but which requires an improvement in its sensitivity by means of an optimized configuration in order to free up new therapeutic perspectives.
Modeling and inclusion criteria
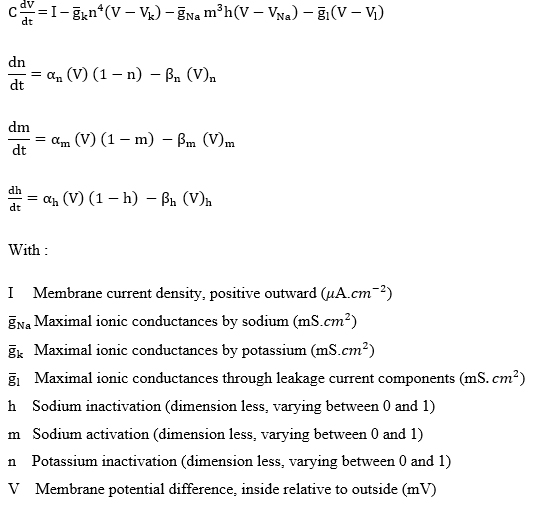
This is a simulation study of the functional brain mapping with a comparative retrospective analysis, has been done by neuronal computational modeling below based on the conductance of Hodgkin Huxley formalism and simulated algorithm by Matlab R2018a (license number 40457466).
The comparison data used are those of cases patients with low-grade glioma tumor have been operated on by common neurosurgical intervention in awake condition, in the Neurosurgery Department of Ibn Sina University Hospital Centre Suissi Rabat, under ethical conditions. The functional brain mapping was produced by Direct Electrical Stimulation (DES) after validation of the speech therapist for each task requested.
Functional brain mapping
DES causes a disorganization of neuron electrical activities located between anode and cathode (5 mm) of the bipolar electrode to force the current to propagate in one direction only. So, it is more focal than the monopolar stimulation. The mapping by DES was obtained by applying a biphasic current of the bipolar electrode verifying the parameters of Table 1, especially 1 to 6 mA for local anesthesia and 4 to 18 mA general anesthesia. It can be controlled by either voltage or current as the parameter of optimization for the brain. Indeed, intensity is the crucial parameter for the neurons activation because in the voltage controlled case stimulation, the intensity delivered cannot be directly monitored since it depends on the stimulated environment (of unknown resistivity, Ohm's law) [1,2] (Figure 1).
Figure 1. (a) Profile of current lines diagram of a bipolar electrode (5 mm). (b) DES parameters used during awake brain surgery
Table 1. Threshold intensities simulation triggering the first action potential in blue
Stimulation
intensity (mA) |
Action potential* (mv) |
Normal structure |
Gray matter+CSF |
White matter+CSF |
2.3 |
6,7406 |
1,1502 |
0,7219 |
2.4 |
103,5505 |
1,2185 |
0,7625 |
5.3 |
108,3723 |
5,5089 |
2,3126 |
5.4 |
108,4128 |
108,9423 |
2,3851 |
7.0 |
108,917 |
110,6449 |
4,4011 |
7.2 |
108,965 |
110,6997 |
5,7114 |
7.3 |
108,9859 |
110,7276 |
109,7669 |
7.4 |
109,0096 |
110,7514 |
110,0994 |
*p=0.0001; CFS: Cerebro Spinal Fluid
Bipolar stimulation threshold in biphasic current
The processing and analysis of simulation data in correlation with the optimization of DES parameters enabled the development of this study, which the results reveal a positive correlation between the DES thresholds optimization and the complete recovery of neurological deficits.
Electrode charge density: The simulation algorithm was able to frame a threshold intensity between (2.3-2.4 mA) and the plot of the charge density in terms of intensity shows an evolution having the appearance of a linear function formulated by equation: y = 0.053 x + 0.008. Thus, for a stimulation threshold of 2.4 mA, the charge density between the two poles of the electrode will be 2.25 mC/cm2 (Figure 2).
Figure 2. Charge density distribution between anode and cathode of the stimulation electrode
Stimulation threshold intensity: Statistical study of the means threshold for each patient reveals a difference in mean of intensity (0.97 mA) in stimulation threshold between the cognitive (1.335 mA) and sensorimotor areas (2.305 mA). Thus, compliance with DES optimization parametrs made it possible to have less fluctuating optimum thresholds explaining the minimum in occurrence frequency of partial or total convulsive seizures. Thus, Figure 3 highlights the simulation effect of 3 rectangular pulse intensities framing the minimum safe stimulation threshold at 2.4 mA [3].
Figure 3. Effect simulation of 3 rectangular pulse currents on action potential
Resistivity effect of Cerebro Spinal Fluid CSF on threshold stimulation
As shown in Table 1, the threshold stimulation intensity in sensory motor cortical area was 2.4 mA. However, the presence of the CSF increases the resistivity of the stimulated structure in the gray than in the white matter, which justifies a marked increase in threshold intensities for these two compartments respectively at 5.4 and 7.28 mA (Figure 4).
Figure 4. (a) Diagram of the action potentials triggered by the threshold intensities of each structure with or without CSF. (b) Evolution of stimulation threshold intensities according to the normal structure, the gray and white matter both with CSF
Stimulation duration
The simulation by frequency standard [50.60 Hz] in the interval [3-5 s] reveals that the threshold stimulation time is 3.1 s. Thus, going towards 5 ms we will get closer to the spikes with an increase in their frequency (Figure 5).
Figure 5. Duration of stimulation Effect on the potential activation
During functional mapping, the stimulation profile used is a biphasic stimulation during a given frequency and duration (pulse duration or pulse width) [4]. The amount of charge injected by a pulse is given by the product of its current intensity and its pulse width (Figure 1). In the biphasic case, the stimulation is balanced when the charges delivered by each pulse are equal [5] to avoid damage to the neural tissues and electrodes (Figure 2).
Optimizing the functional mapping as specific technique requires precise configuration of the DES for improving its sensitivity linked to false negative, when the DES of an area did not cause an intraoperative deficit (negative mapping), while its surgical excision causes a permanent neurological deficit.
Indeed this boundary condition is due to the stimulation by an intensity lower than 2,4 mA the threshold intensity (Figure 3) or a short stimulation period beyond the threshold of 3.1 s to 5 s (Figure 4) and stimulation during the refractory period of a post-discharge operating hyperexcitability [6].
Also, a CSF abundance in the mapping site increases by factor of 4 and 6 respectively the gray and white matter resistivity (Figure 5). [7,8]
A specific mapping by DES without false negative remains a very promising path for improving the sensibility around 100% to operate with very high functional safety.
Therefore, optimization of stimulation thresholds will not induce or minimize the effect generated by its antidromic propagation along the axons towards a truly essential network, and/or the functional compensation of the area stimulated by neuroplasticity mechanisms [9] (Figure 6).
Figure 6. Effect of current lines in cortical stimulation. Generation mechanism of Direct cortical response (DCR) and cortico axono cortical evoked potential (CACEP) like in deeper stimulation
As shown in Figure 7, the success of awake surgery depends on the functional mapping quality which is a function of the DES in optimized thresholds improving the sensitivity of this specific technique.
Figure 7. Range of use and safety of DES according to intensity applied by bipolar electrode (5 mm inter-distance electrode)
Improving the functional mapping quality means overcoming the effect of boundary conditions affecting its sensitivity under the false negative impact without forgetting the manageable impact of false positives on its specificity. Thus, under the beneficial effect of the parameters optimization acting on the sensitivity, the awake surgery becomes not only a revolutionary technique; because of the extent of the resection, which is currently done according to functional imperative, unlike the onco-anatomical limits during the classical paradigm; but to free up new therapeutic perspective towards a functional, personalized and maximalist surgical neuro-oncology without malignant transformation.
The data [Exploitation sheet, Clinical informations] used to support the results of this study are available upon request from the corresponding author.
The data used to support the findings of this study are included within the article.
There are no conflicts of interest regarding the publication of this paper.
- Vincent M, Rossel O, Hayashibe M, Herbet G, Duffau H, et al. (2016) The difference between electrical microstimulation and direct electrical stimulation- towards new opportunities for innovative functional brain mapping? Rev Neurosci 27: 231-258. [Crossref]
- Warman EN, Grill WM, Durand D (1992) Modeling the effects of electric fields on nerve fibers: determination of excitation thresholds. IEEE Trans Biomed Eng 39: 1244- 1254. [Crossref]
- Bouadel A, Oudrhiri MY, El Hassani M, Kabbaj S, Jiddane M, et al. (2019) Functional brain mapping optimization during awake craniotomy. Trends Med 20: 5-5.
- Merrill DR, Bikson M, Jefferys JG (2005) Electrical stimulation of excitable tissue: design of efficacious and safe protocols. J Neurosci Methods 141: 171-198. [Crossref]
- Rattay F (1999) The basic mechanism for the electrical stimulation of the nervous system. Neuroscience 89: 335-346. [Crossref]
- Jayakar P (1993) Physiological principles of electrical stimulation. Adv Neurol 63: 17-27.
- Geddes LA, Baker LE (1967) The specific resistance of biological material—a compendium of data for the biomedical engineer and physiologist. Med Biol Eng 5: 271-293.
- Nathan SS, Lesser RP, Gordon B, Thakor NV (1993) Electrical stimulation of the human cerebral cortex. Theoretical approach. Adv Neurol 63: 61-85.
- De Witt Hamer PC, Robles SG, Zwinderman AH, Duffau H, Berger MS (2012) Impact of intraoperative stimulation brain mapping on glioma surgery outcome : a meta-analysis. J Clin Oncol 30: 2559-2565.