Abstract
Introduction: Obesity is a chronic disease of multifactorial etiology. It is prevalence is increasing in epidemic form in the last decade, favoring the occurrence of various metabolic disorders such as type 2 diabetes mellitus and dyslipidemia, involving the increased morbidity and mortality. Objective: Evaluate weight loss and metabolic profile in patients in follow up at obesity clinic with nutritional education or medication. Method: The study realized the evaluation of medical records of 95 patients from Obesity Group ambulatory and analysis their metabolic profile. Obesity was defined as body mass index greater than or equal to 30 kg / m2. It was set at 0.05 or 5% (α ≤ 0.05) level to reject the null hypothesis. Results: There was 95 patients, with age around 45 years, prevalence in woman, with significance loss weight and got better metabolic profile. Mean weight loss of 7% in the group with medication and 3.1% without medication. There were significant reductions in weight and glycated hemoglobin, TC, TG, LDL. Conclusion: Our study demonstrated the metabolic aspects of obese adults and a significant improvement in weight loss and nutritional education and outpatient treatment with specialized professional group.
Introduction
Obesity is a multifactorial syndrome in which genetics, metabolism and environment interact, assuming different clinical pictures, in different socio-economic realities. Currently, it is considered a condition of high prevalence, which raises the attention of the clinician, researcher, and professionals social [1].
The obesity diagnosis is defined as a body mass index (BMI) greater or equal to 30 kg/m2, which is usually accompanied by other comorbidities such as diabetes mellitus, dyslipidemia and hypertension [1-3].
The increasing prevalence of overweight and obesity in the population was observed from epidemiological studies and can be attributed in part to increased access to processed foods, lack of adequate information that leads to bad eating habits and also to changes in style life and eating habits. The overweight in 2003 reached 40% of the adult population, and the prevalence of obesity for men was 8.9% and 13.1% among women [2].
The frequency of obesity varies according to gender, age, race and socio-economic conditions. Epidemiological data indicate an increase in the prevalence of obesity in European countries, the US and most other countries. In Brazil, it is estimated that 26.5% of women and 22% of men have excess weight, 11.2% of women and 4.7% of men have mild obesity and 0.5% of women and 0.1% of men have class III obesity [2,3].
The presence of comorbidities such as diabetes mellitus, hypertension and dyslipidemia are usually present in the obese, providing a cardiovascular risk more acentuado [1,2].
It is known that the treatment of obesity is complex and depends on a multidisciplinary team, and fundamental change in eating habits, guidance for physical activity, limited drug therapies, behavioral therapy and surgery bariatrica [1-4].
In this context, it justifies our interest in evaluating the therapy related to obesity group and analyze not only weight loss, but whether there was significant change in the metabolic profile of the obese patient.
Objective
Evaluate weight loss and metabolic profile in patients in follow up at obesity clinic with nutritional education or medication.
Method
This is a retrospective, analytical study, which was approved by the Research Ethics Committee of Irmandade Santa Casa de Misericordia de Sao Paulo.
The study realized the evaluation of medical records of 95 patients from Obesity Group ambulatory at Irmandade Santa Casa de Misericordia de São Paulo in a period of six months. Obesity was defined as body mass index greater than or equal to 30 kg/m2
The Obesity Group has a nutritionist who accompanies patients every three months to carry out the nutritional education, and in the first time is held a talk with the endocrinologist with a group of up to 20 patients at a time to clarify the obesity harms and the importance of their treatment. Consultations at the clinic with endocrinologist is performed quarterly.
Inclusion criteria: BMI greater than or equal to 30 kg/m2, older than 18 years. Exclusion criteria: performing bariatric surgery.
The anti-obesity drugs (orlistat and sibutramine) are prescribed in specific cases, which the patient can no significant weight reduction and when does not have coronary artery disease, hypertension or when it has 60 or more in the case of the second drug. It is noteworthy that the cost of treatment is a limiting factor for most patients.
The metabolic profile was assessed with serum levels of glycated hemoglobin, total cholesterol, LDL and triglycerides. A collection of tests occur at the first visit and 'and assessed the collection after a period of nine months.
They were evaluated: weight, age, body mass index (BMI), gender, age for epidemiological analysis. Individuals present quarterly monitoring which are verified weight and height on the same machine. Statistical analysis was performed using Epi-info software, version 6.0 and Wilcoxon test for paired measures, considering significant result p<0.05.
Results
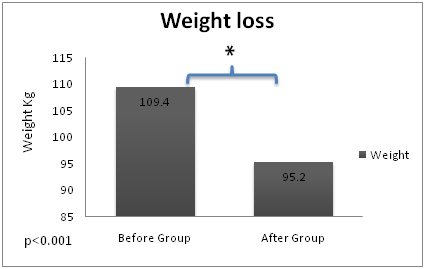
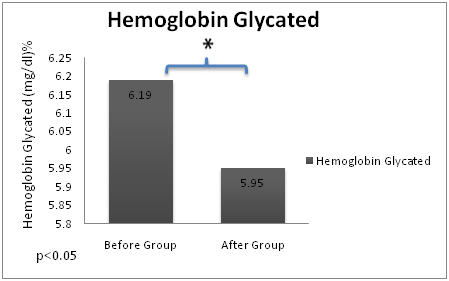
There were 95 patients, 82 women and 13 men with a mean age of 45.7 years. The general comparison of the weight of groups before (WB) and after (WA) nutricional education and the average glycated before the group (GB) and after the group (GA) can be described in graph 1 and 2. During analysis, we separated patients who used or not medication to better detailment the differences in the treatment group. The results about metabolic profile were more favorable in the group that used medication, but in relation the weight, the loss was important in both. The evolution of patients who used medications to aid weight loss can be observed in Table 1, and not medication in Table 2.
Table 1. Metabolic profile before and after group with medication
|
|
Before group
|
SD
|
After group
|
SD
|
p
|
|
Wheight
H. glycated
Cholesterol
LDL
TG
|
105.5
6.41
193.9
117
150
|
27.3
1.5
30
27.4
55.5
|
98.2
6.08
181.7
109
133.1
|
17.8
1.54
30
27.2
54.6
|
0.001
0.024
0.005
0.003
0.001
|
H. glycated: hemoglobin glycated, Cholesterol: total cholesterol, TG: triglycerides
Table 2. Metabolic profile before and after group without medication
|
|
Before group
|
SD
|
After group
|
SD
|
p
|
|
Wheight
|
101.2
|
18.8
|
94.1
|
18.6
|
0.001
|
|
H. glycated
|
5.96
|
1.03
|
5.81
|
1.05
|
0.092
|
|
Cholesterol
|
178.5
|
33.6
|
171
|
32
|
0.817
|
|
LDL
|
116.1
|
31.2
|
109
|
30.8
|
0.174
|
|
TG
|
149.3
|
65.6
|
136
|
50.1
|
0.004
|
H. glycated: hemoglobin glycated, Cholesterol: total cholesterol, TG: triglycerides
2021 Copyright OAT. All rights reserv
Discussion
It is known that obesity is a pandemic with significant financial and clinical implications. Studies has demonstrated the interaction of genetic and environmental factors, including socio-cultural factors, nutrition, smoking, alcohol consumption and physical activity [5].
The current treatment of obesity is characterized as a challenge, in that there is a need for action of a team multidisciplinar. As demonstrated in this article, another study with 270 participants also proved that. In a period of two years intensive multidisciplinary treatment was successful in responding to the treatment of obesity. Advanced age, obesity up to grade III and financial aid were baseline characteristics of this study. In this sense, we have made a multidisciplinary approach and close monitoring in an ambulatory specifically targeted obesity, with the initiative of forming a group involving patients, medical and nutritionist [6-8].
There are several ways to study the best way of treating obesity mainly because of the numerous comorbidities generated by this disease, with high rate of morbidity and mortality. In this context, a study linking literacy with regard to obesity specifically, a systematic orientation, was executed, considering that more disadvantaged people have high overweight index, as well as in our study. However got no significant difference in the control group, being highlighted the lack of sufficient evidence to determine the relative effectiveness of individual interventions [9,10].
Our ambulatory is inherent in the single health system, which comprises a poorest socioeconomic profile. The scarcity of studies measuring socioeconomic status should be addressed in future research, given the obesity rates are higher in disadvantaged population groups [9].
It is known that weight loss provides improved metabolic profile progressively reducing the risk of co-morbidities aggravation. Our study emphasized the weight loss knowledge that provides a significant reduction in blood glucose and lipid profile and blood pressure values [7-10].
We consider important to share methods in the treatment of obesity because this disease has been difficult to adhesion, because it requires behavioral changes from patient. Hence our interest in promoting our group of experts and our results.
We understand that the presence of professionals from the fields of psychology and physical education provide a much more significant impact improvement. However, we do not have available [10].
The quarterly monitoring by the Obesity Group (nutritionist and endocrinologist with meetings) triggered a significant improvement in metabolic profile and weight loss characterized as therapeutic success.
Conclusion
This study aims to emphasize the metabolic aspects of obese adults and a significant improvement in weight loss and nutritional education and outpatient treatment at a specialty.
References
- Abate N, Garg A, Peshock RM, Stray-Gundersen J, Grundy SM (1995) Relatioships of generalized and regional adiposity to insulin sensitivity in men. J Clin Invest 96: 88-98. [Crossref]
- WHO (2000) Obesity: preventing and managing the global epidemic. Report of a WHO consultation. Technical Report Series. Geneva. World Health Organization, 2000. Report n 894
3.Atualização das diretrizes para o tratamento Farmacológico da obesidade e do sobrepeso. Posicionamento Oficial da ABESO / SBEM -2010 –
- Wadden TA, Berkowitz RI, Womble LG, Sarwer DB, Phelan S, et al. (2005) Randomized trail of life style modificationand pharmacotherapy for obesity. N Engl J Med 353: 2111-20. [Crossref]
- Cataneo C, Carvalho AMP, Galindo EMC (2005) Obesidade e Aspectos Psicológicos: Maturidade Emocional, Auto-Conceito, Locus de Controle e Ansiedade. Psicologia: Reflexão e Crítica 18: 39-46.
- Barros CASM, Werutsky CA, Gütfriend C, Biernat ES, Barros TM (1990). Transtorno da imagem corporal de obesos em grupoterapia. Revista de Psiquiatria do Rio Grande do Sul 12: 75-83.
- Ben-Tovin DI, Walker MK (1994) The influence of age and weighton womens body attitudes as measured by the body attitudes questionnaire (BAQ). J Psychosomatic Res 38: 477-481. [Crossref]
- Rothberg AE, McEwen LN, Kraftson AT, Ajluni N, Fowler CE, et al. (2015) Factors associated with participant retention in a clinical, intensive, behavioral weight management program. BMC Obes 2: 11. [Crossref]
- Faruqi N, Spooner C, Joshi C, Lloyd J, Dennis S, et al. (2015) Nutrients. Primary health care-level interventions targeting health literacy and their effect on weight loss: a systematic review 7: 5868-5888.
- Elbelt U, Schuetz T, Knoll N, Burkert S (2015) Self-directed weight loss strategies: energy expenditure due to physical activity is not increased to achieve intended weight loss. Nutrients 7: 5868-5888. [Crossref]