Antiphospholipid syndrome(AS) or antiphospholipid body syndrome is associated with arterial or venous thrombosis. This syndrome is diagnosed with determining serum antiphospholipid bodies which lead to the clinical events such as arterial or venous thrombosis [1-10]. Pathophysiology of disease is associated with activating coagulation cascade or inhibiting protein S and/or protein C by antiphospholipid bodies. Besides all the arterial system occlusion, thrombotic occlusion of the coronary artery vessels is very important which lead to life threatening events.
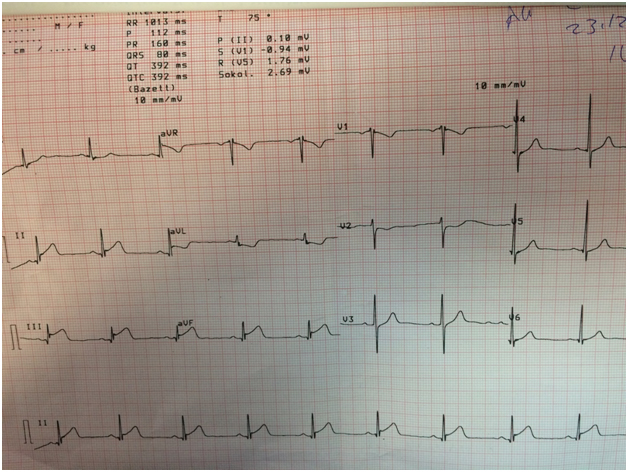
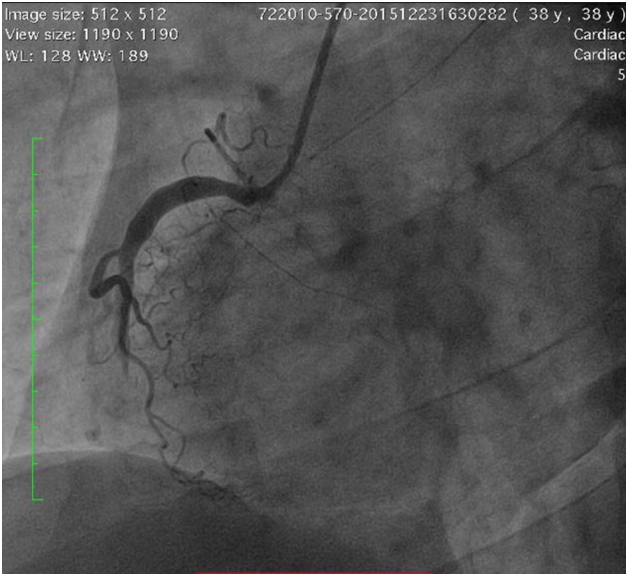
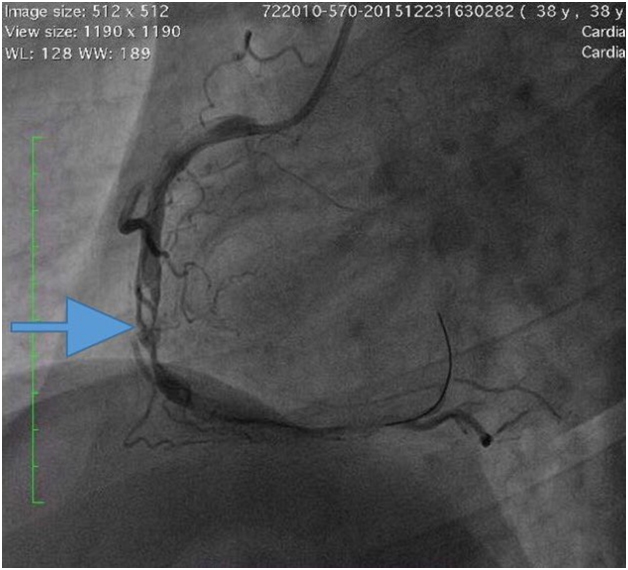
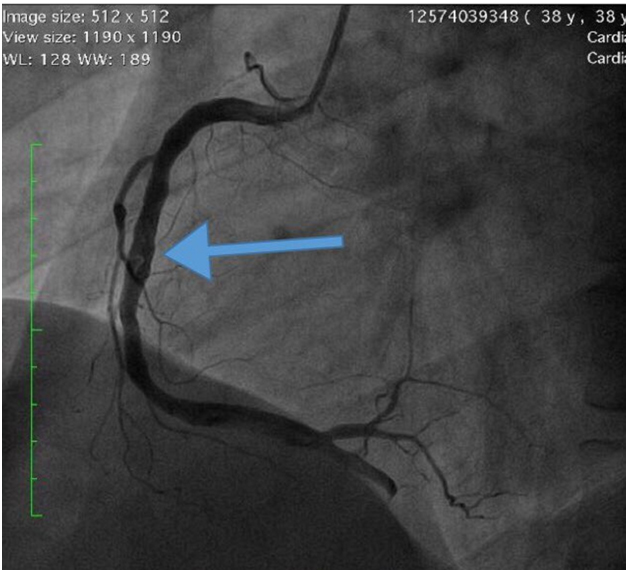
Herein, we report a 38 year old man with histories of antiphospholipid syndrome and pulmonary thromboembolism who presented with acute chest pain for 4 hours was admitted to our coronary care unit. He was advised warfarin therapy before but he did not use warfarin or any other drugs. He has left his warfarin therapy for over a month. There were ST segment elevation on inferior derivations and reciprocal changes D1-aVL derivations on electrocardiogram(Figure-1). High sensitive troponin T level was significantly elevated. Physical findings were not remarkable. The patient was diagnosed to have a acute inferior ST-elevation myocardial infarction(STEMI) and was transferred to the catheter laboratory. Dual anti-platelet therapy(acetylsalicylic acid and clopidogrel) was initiated. Invasive coronary angiography showed a total occlusion of the right coronary artery(RCA) after right ventricular side branch(Figure-2). There were no significant stenosis on the left anterior descending artery and circumflex artery. LVEF was 50% and severe hypokinesia of the inferior and apical wall of the left ventricle was detected on transthoracic echocardiography. A o.o14 inches floopy wire and 3.0x15 mm balloon were inserted to the to RCA and was inflated several times. The TIMI-2 flow was obtained with balloon inflation but there was severe thrombus formation through the vessel(Figure-3,Video-1). We applied intracoronary tenekteplase, intravenous heparin and abciximab infusions for 24 hours in additon to aspirin and clopidogrel treatment. The patient was transferred to the coronary care unit. After 24 hours, control coronary angiogram showed severely diminished but persistent thrombus formation on distal part of the RCA with adequate flow(Figure-4, Video-2). Warfarin was started with dual antiplatelet treatment. When INR was 2, the patient was discharged with no complication and segmental wall motion abnormality.
Figure 1: The 12-lead electrocardiogram of the patient.
Figure 2: First angiographic view of the occluded RCA.
Figure 3: Angiographic view of the RCA after balloon inflation.
Figure 4: Angiographic view of the RCA after 24 hours.
In conclusion, high thrombus burden in patients with AS may cause total occlusion of the coronary vessels. Aggressive antithrombotic treatment in additon to the balloon inflation is feasible in case of low bleeding risk as in our young case and it should be preferred rather than stenting. The triple therapy must be added to the medication in young patients with low bleeding risk.
References
2021 Copyright OAT. All rights reserv
Raddino R, Pedrinazzi C, Zanini G, Procopio R, Dei Cas L (2005) Acute myocardial infarction in a young woman with antiphospholipid syndrome and occasional cocaine abuse.Int J Cardiol 105: 236-238. [Crossref]
Sajeev CG, VivekNambiar K, Fasaludeen M, Jayakumar TG, Krishnan MN, et al. (2003) Myocardial infarction in a young woman with antiphospholipid syndrome.Int J Cardiol 91: 99-100.[Crossref]
Gotsman I, Mosseri M (2005) Acute myocardial infarction in a young women with normal coronary arteries and a combined thrombophilia.Int J Cardiol 99: 483-484. [Crossref]
Umesan CV, Kapoor A, Nityanand S, Tiwari S, Sinha N (1999) Recurrent acute coronary events in a patient with primary antiphospholipid syndrome: successful management with intracoronary stenting. Int J Cardiol71: 99-102. [Crossref]
Martí V, Seixo F, Santaló M, Serra A (2014)Antiphospholipid syndrome and acute myocardial infarction: treatment with thrombectomyandabciximab. Rev Port Cardiol33:465.e1-4. [Crossref]
Martí V, Seixo F, Santaló M, Serra A (2015) Recurrent acute myocardial infarction as an initial manifestation of antiphospholipidsyndrome:treatment and management. Blood Coagul Fibrinolysis 26:91-94. [Crossref]
Maor E, Fefer P, Varon D, Rosenberg N, Levi N, et al. (2015) Thrombophilic state in young patients with acute myocardial infarction. J Thromb Thrombolysis 39: 474-480. [Crossref]
Balta I, Balta S2, Demir M3, Ozturk C2, Demirkol S3 (2015) Thrombosis with Behçet's disease should be evaluated different conditions.Pan Afr Med J 20: 117. [Crossref]
Karadurmus N, Oztürk C, Sönmez A, Dogru T, Inal S, et al. (2008) Combined heterozygote factor V Leiden mutation and anticardiolipin antibody positivity in a young patient with spontaneous deep vein thrombosis. AnadoluKardiyolDerg8:71-73. [Crossref]
Iyisoy A, Kursaklioglu H, Kose S, Yesilova Z, Ozturk C, et al. (2004) Acute myocardial infarction and left subclavian artery occlusion in Behçet's disease: a case report.Mt Sinai J Med 71: 330-334.[Crossref]
Editorial Information
Editor-in-Chief
Dario Marchetti
Baylor College of Medicine
Article Type
Case Report
Publication history
Received: February 19, 2016
Accepted: February 25, 2016
Published: February 29, 2016
Ozturk C, Yildirim AO, Demir M, Balta S, Celik T,et al.(2016). Acute inferior myocardial infarction with severe thrombus formation in a young male patient with primary antiphospholipid syndrome.Gen Int Med ClinInnov1: doi:10.15761/GIMCI.1000107
Corresponding author
Cengiz OZTURK
Associate Professor of Cardiology, Department of Cardiology, Gulhane School of Medicine, TevfikSaglam St., 06018 Etlik, Ankara, Turkey, Tel: +903123044264, Fax: +903123044250.