An asymptomatic 75-year-old female with past medical history of percutaneous coronary intervention for angina pectoris was referred to our department for the management of left ventricular aneurysm which was pointed out on the follow-up echocardiography. Coronary angiography revealed no restenosis of the stent site, but 100% stenosis of a distal segment of the left circumflex artery that had not been detected previously. Transthoracic echocardiography indicated a defect of the myocardium 2cm in diameter in the posterior wall Aneurysmectomy and patch closure was performed successfully before rupture and the lesion was diagnosed as subepicardial aneurysm.
aneurysm (left ventricle), myocardial infarction
Subepicardial aneurysm of the left ventricle is a rare but lethal complication of myocardial infarction. It is classified as subtype of incomplete myocardial rupture. Its features include abrupt interruption of the myocardium, a narrow neck, and propensity for progression to sudden trans-luminal rupture. This etiology has not been well reported because of its rarity and difficulty in diagnosis before rupture. Management has not defined but surgical repair is the only therapy to prevent rupture. We report a case of asymptomatic SEA incidentally pointed out on echocardiography and successfully treated by surgery. The etiology, clinical presentation, diagnosis, imaging findings and management are here discussed. We should keep in mind this condition as a life-threatening complication of myocardial infarction with the risk of trans-luminal rupture, even if asymptomatic.
An asymptomatic 75-year-old female with past medical history of percutaneous coronary intervention for angina pectoris and chronic renal failure on hemodialysis was referred to our department for the management of left ventricular aneurysm which was pointed out on the follow-up echocardiography. Coronary angiography showed no restenosis of the stent site but 100% stenosis of distal segment of left circumflex artery which had not been detected previously. Echocardiography showed an abnormal cavity that communicated with the left ventricle through a small hole, 2cm in diameter in the lateral wall (Figure 1). Figure 2. Computed tomography scan showed an aneurysm in the lateral wall of left ventricle without pleural effusion (Figure 2). Magnetic resonance imaging showed an aneurysm with abrupt discontinuing of myocardium and narrow neck (Figure 3). Pseudoaneurysm, subepicardial aneurysm or pseudo-pseudoaneurysm was thought as differential diagnosis. Aneurysmectomy and patch closure was planned. Surgery was performed via medial sternotomy. Cardiopulmonary bypass (CPB) was carried out with cannulation of the aorta and the right atrium under cardiac arrest and mild hypothermia. Macroscopically, a subepicardial little red aneurysmal site with a weakened wall was seen at the apical part of the left ventricle. Sign of rupture, adhesion to the surrounding structures or pericardial effusion was not seen. The aneurysmal sac was opened and a sclerotic wall was seen. There was a narrow neck at the base of the incised aneurismal sac communicating with the left ventricular cavity. Myocardium was not contained in the aneurysm cavity (Figure 4). Following the resection of the aneurysm, the defect was patch closed with Gelweave graft. Two Teflon pledgets were used to reinforce the ventricle suture on the outside. The weaning from CPB and postoperative course were uneventful.
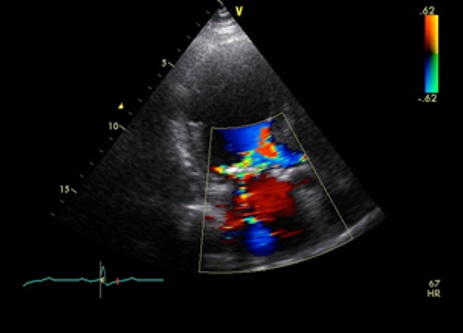
Figure 1. Transthoracic echocardiography showed abrupt myocardial interruption in the inferior wall. The aneurysm was 16mm×20mm in size without external expansion.
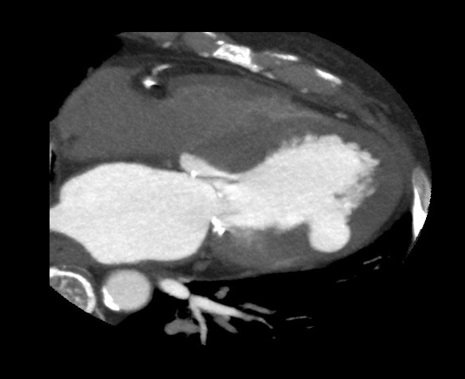
Figure 2. Computed tomography scan showed an aneurysm lying below the inferior surface of left ventricle without pleural effusion.

Figure 3. Magnetic resonance imaging showed an aneurysm below the inferior surface of the left ventricle with abrupt discontinuing of myocardium and narrow neck.
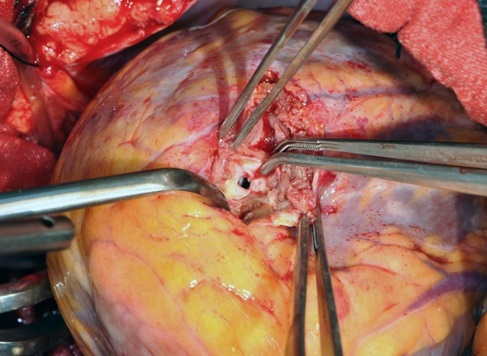
Figure 4. Intraoperative picture showed that aneurysm had a narrow neck and myocardium was not contained in the aneurysm cavity.
Cardiac rupture, whether complete or partial, is a potentially lethal mechanical complication of myocardial infarction. Subepicardial aneurysms, pseudoaneurysms and pseudo-pseudoaneurysms represent three rare varieties of incomplete cardiac rupture [1-6]. In 1983, Epstein and Hutchins defined subepicardial aneurysm of the left ventricle as a rare complication of myocardial infarction [7]. Vossenberg et al. reported that the overall incidence of subepicardial aneurysms ranges from 0.3% at consecutive autopsy series to 1% of myocardial infarction deaths [8]. Subepicardial aneurysms are characterized by an abrupt interruption of the myocardium opening to an aneurysmal pouch that is contained by epicardium and may also contain myocardial elements. Although rare, subepicardial aneurysms have several unique characteristics with important clinical implications. First, subepicardial aneurysms have been associated with a high risk of rupture [9-12]. The potential to rupture is high both in the early stages of development and in the chronic phase [13,14]. Second, they are also associated with other significant cardiac morbidity such as moderate-severe congestive heart failure, ventricular septal defects, true aneurysm formation, mitral regurgitation, ventricular arrhythmias, systemic emboli [7]. Finally, prompt recognition and surgical repair offers a favorable prognosis. Vossenberg et al reported a literature review of 16 aneurysms, in which 31% had ruptured. Sixteen cases of subepicardial aneurysm (80%) were described as having occurred in the inferior or posterior walls, two (10%) in the anterolateral wall, one (5%) in the anteroseptal wall, and one (5%) involving the apex [8]. Six (30%) progressed to frank rupture. In six patients, the diagnosis was made only at autopsy. Ante-mortem diagnosis was made in 14 patients, 12 of whom underwent operative repair [11]. Although appropriate timing for surgical treatment remains unclear, an increase in size and external expansion of subepicardial aneurysm, which would be the anatomical indicator of rupture, require urgent surgery. Even if external expansion does not occur, surgical correction is necessary because of possible progression. To prevent to progression to rupture, serial echocardiography should be performed to detect the formation of aneurysm, increase in size and external expansion of a subepicardial aneurysm [15-17]. In conclusion, we should keep in mind this condition as a life-threatening complication with the risk of transluminal rupture, even if asymptomatic. Serial echocardiography follow-up should be performed following myocardial infarction to detect the formation of aneurysm, increase in size and external expansion of a subepicardial aneurysm. Once it is diagnosed, prompt surgical intervention should be considered before rupture.
All the authors have declared no competing interest.
- Atik FA, Navia JL, Vega PR, Gonzalez-Stawinski GV, Alster JM, et al. (2007) Surgical treatment of postinfarction left ventricular pseudoaneurysm. Ann Thorac Surg 83: 526-531. [Crossref]
- Narin C, Ege E, Ozkara A, Tanyeli O, Sarkilar G, et al. (2008) Surgical treatment of postinfarction pseudoaneurysms of the left ventricle. J Card Surg 23: 294-298. [Crossref]
- Frances C, Romero A, Grady D (1998) Left ventricular pseudoaneurysm. J Am Coll Cardiol 32: 557-561. [Crossref]
- Gollol-Raju N, Olearczyk B, Johnson R, Menzies DJ (2007) Pseudo-pseudoaneurysm: a rare and unexplored mechanical complication of myocardial infarction. J Am Soc Echocardiogr. 20: 1317.e1-3.
- Lakkireddy DR, Khan IA, Nair CK, Korlakunta HL, Sugimoto JT (2005) Pseudo-pseudoaneurysm of the left ventricle: a rare complication of acute myocardial infarction--a case report and literature review. Angiology 56: 97-101. [Crossref]
- Singh BK, Greene AL, Ritchie ME (1998) Pseudo-pseudoaneurysm of the left ventricle. Cardiology 89: 159-161. [Crossref]
- Epstein JI, Hutchins GM (1983) Subepicardial aneurysms: a rare complication of myocardial infarction. Am J Med 75: 639-644. [Crossref]
- Vossenberg F, Amidi M, Kormos R, Labuda MJ (1991) Subepicardial aneurysm of the left ventricle: report of a case and review of the literature. Clin Cardiol 14: 169-172. [Crossref]
- Koito H, Nakamura C, Suzuki J, Kamihata H, Takayama Y, et al. (1999) Pseudoaneurysm of the left ventricle progressing from a subepicardial aneurysm. Jpn Circ J 63: 559-563. [Crossref]
2021 Copyright OAT. All rights reserv
- Giltner A, Marelli D, Halpern E, Savage M (2007) Subepicardial aneurysm with impending cardiac rupture: a case of antemortem diagnosis and review of the literature. Clin Cardiol 30: 44-47. [Crossref]
- Hirota M, Omoto T, Ishikawa N, Fukuzumi M, Ohnomd M (2010) Surgical strategy for subepicardial aneurysm: two case reports. Ann Thorac Cardiovasc Surg 16: 291-293. [Crossref]
- Hayashi T, Ichikawa M, Yutani C, Iwata A, Yamaguchi T, et al. (2009) Echocardiographic progression of a subepicardial aneurysm after inferior myocardial infarction. J Cardiol 54: 339-343.
- Bunch TJ, Oh JK, Click RL (2003) Subepicardial aneurysm of the left ventricle. J Am Soc Echocardiogr 16: 1318-1321. [Crossref]
- Tosun R, Kaplan M, Sanioglu S, Olsun A, Oztek I, et al. (2008) Subepicardial left ventricular aneurysm with an intraventricular narrow neck on the avascular apical area: report of a case. Surg Today 38: 951-954. [Crossref]
- Takeda S, Yonezawa M, Shirasawa K, Hatakeyama Y, Sasaki Y, et al. (2007) Oozing type of left ventricular rupture via subepicardial aneurysm diagnosed 5 months after myocardial infarction. Int J Cardiol 115: e20-1.
- Hironaka E, Kojima S, Hongo M, Fukaya Y, Katagiri Y, et al. (1997) Echocardiographic diagnosis of subepicardial aneurysm ruptured into the right ventricle after inferior myocardial infarction. J Am Soc Echocardiogr 10: 192-196.
- Tanabe K, Sugamori T, Yoshitomi H, Asanuma T, Shimada T (2000) Fatal cardiac rupture: a case of subepicardial aneurysm after myocardial infarction. J Am Soc Echocardiogr 13: 951-952. [Crossref]