Abstract
The nasopalatine duct is an anatomical structure that connects nose to oral cavity. This anatomic area may be affected by a large group of pathologies. In this paper, we reported a very rare case of cholesterol granuloma located in the nasopalatine duct. No other case of nasopalatine localization of a cholesterol granuloma has been reported in literature up to the present time. The Cholesterol Granuloma (CG) is a foreign body reaction due to the deposition of cholesterol crystals. It is very common in the middle ear, although ectopic manifestations can be vary. In the nasopalatine duct CG may simulate other pathological conditions with similar clinical and radiological features, for this reason a careful histological examination is necessary to avoid mistakes and wrong diagnosis.
Key words
cholesterol granuloma, maxillary sinus, nasopalatine duct, oral surgery, oral pathology
Introduction
The nasopalatine duct is a structure that connects nose and oral cavity. The duct generally terminates in the floor of the nasal cavity near the vomeronasal organ [1]. This regionmay beaffected by varioustypes oflesion such as: inflammatory radicular cyst, nasopalatine duct cyst, odontogenickeratocyst, etc [2-4]. The Cholesterol Granuloma (CG) is a foreign body reaction due to the deposition of cholesterol crystals. CG is usually found in association to chronic middle ear diseases; however ectopic manifestations can be seen in other anatomic sites. Rarely, the paranasal sinuses may be involved and it seems to be due to impairment of drainage, disturbed ventilation and hemorrhage into the sinuses with hemolysis [5]. CG is more common in the middle age, and it also has a predilection for male gender with a ratio male/famale of 3:1 [6]. Trauma and bleeding are considered the most important ethiopatogenic event for CG development. In fact, the cholesterol, present into the lesion, probabily derive to the cell membrane of erythrocytes destroyed during bleeding, they also precipitates in a crystalline form caused by an inadequate drainage [7]. The connective tissue degeneration seems also play a role, because it is associated with a reduction of ventilation, caused by osteomeatal complex obstruction by trauma and inflammatory products [8]. The presence of CG in the maxillary sinus is well reported in literature with about 40 cases reported, however the incidence could be higher, because of mistakes in the diagnosis [9]. Nasopalatine involvement for CG is very rare and is not reported in the current literature. In this case, we report a case of CG that simulates a nasopalatine duct cyst.
Case report
A 53-years-old man referred at Dental Clinic of the University of Foggia for the evaluation of a bulge in the anterior region of the palate (Figure 1). The patient didn't present systemic pathologies and there was not history of trauma. At the general anamnesis, the patient declared to not suffer of any disease, to not assume drugs and that he had never been allergic to any substance. The lesion turned out fully painless and soft at the clinical palpation. All teethwere found tobe vitalandrespond negativelyto thetestofpulp vitality and percussion. No other dental sign were present with the exception of an old amalgam reconstruction on the element 2.6. An orthopanoramic (OPT) (Figure 2) and a computed tomography (CT) dentascan (Figure 3) were prescribed and the patient was returned to control visit after a week. Ortopantomography showed a well-defined radiolucency approximately 1.5 cm in size with corticated margins in the midline between the central incisors. CT scan also showed a well-defined radiolucency in anterior maxilla in the region of incisive canal, 1.4 cm x 1.2 cm in size. Surgical operation was carried out after two weeks.A surgical incision from element 1.5 to 2.5 was performed after a previous local anesthesia (Figure 4), soafull-thickness flap was raised to allow the exposure of the lesion. The bulk was cleavage through the use of a hemostatic forcepsand a periosteal elevator. A surgical enucleation was done with intact removal of the lesion and the specimen was sent to the pathologist for the histopathological examination (Figure 5). Afterwards, acarefulcurettageof theresidualcavityhad performed and so followedbyasurgicalinterrupted suture (Figure 6). Histological sections stained with hematoxylin and eosin showed a connective tissue containing extensive areas of cholesterol clefts, surrounded by multinucleated foreign body giant cells, chronic inflammatory cells, macrophages and foam cells (Figures 7 and 8). Histological examination revealed the diagnosis of cholesterol granuloma.

Figure 1. Looking the hard palate it's possible to notice the presence of a bulk which led to a bulge of the papilla
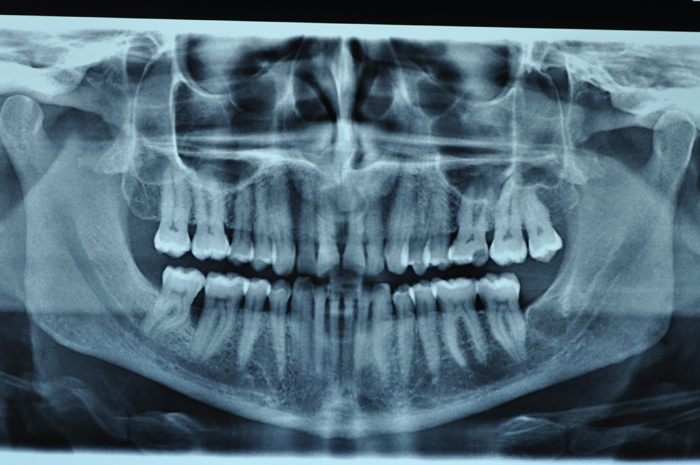
Figure 2. OPT revealed the presence of an osteolytic lesion between the maxillary central incisors
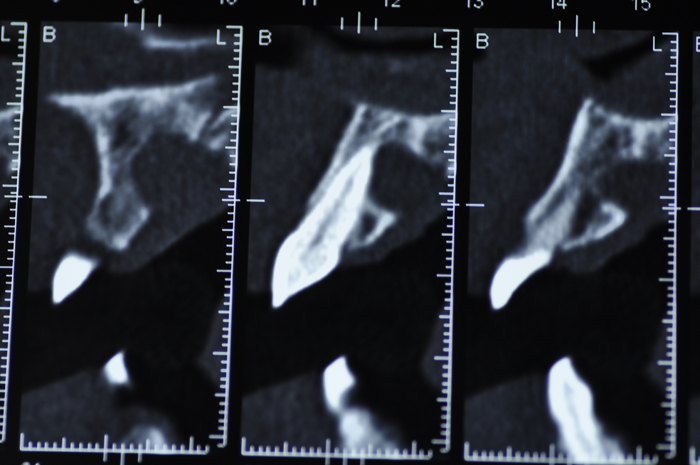
Figure 3. CT-scan showed a well-defined radiolucency approximately 1.5 cm in size, with a clear erosion of the palatal bone cortex.
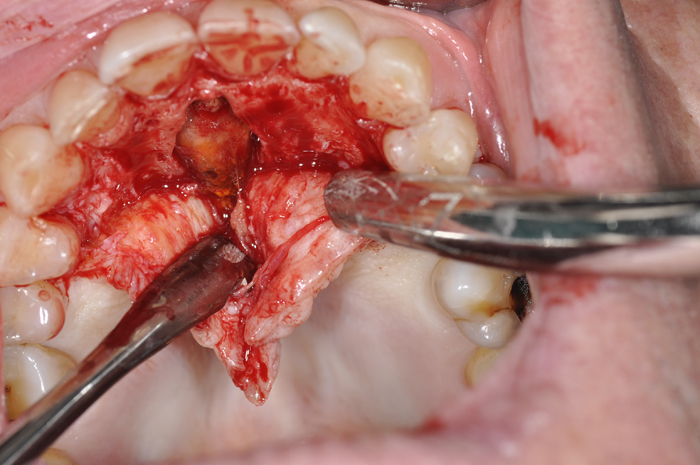
Figure 4. A full-thickness intrasulcular surgical incision was perfomed from the tooth 1.5 to the element 2.5

Figure 5. The lesion resulted in a complete erosion of the cortical palatal and appeared in connection with the connective tissues
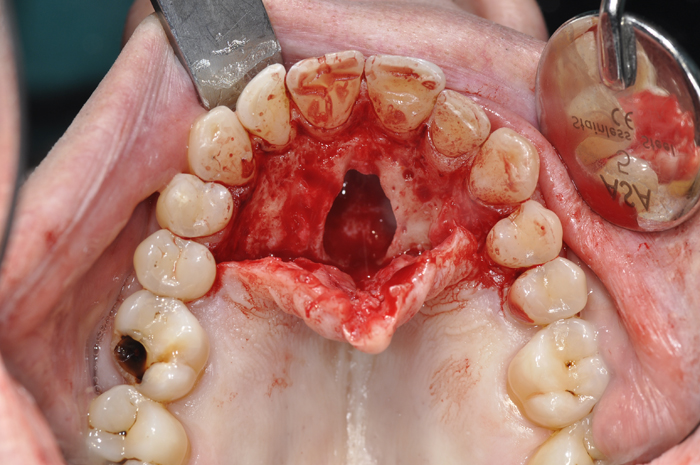
Figure 6. Cleavage and enucleation were performed avoiding an injury of the nasopalatine nerve


Figures 7 and 8. Histological examination stained with hematoxylin and eosin showed a connective tissue containing extensive areas of cholesterol clefts.
Discussion
Herein, we reported a case of cholesterol granuloma located in the nasopalatine duct. CG is a foreign body reaction due to the deposition of cholesterol crystals, usually found in association to chronic middle ear diseases [6]. CG has been found in many body areas such as: ear (its most common site), mastoid process, breast, sellaturcica, pancreas, testis, lungs, brain and kidneys and in the apex of the temporal bone pyramid. There is a prominent sex predilection for males, and a racial difference with Caucasians and Turkishs who more frequently suffer for CG [9]. Possible mechanisms involved in the pathogenesis of maxillary sinus CG are impairment of drainage, disturbed ventilation and hemorrhage into the sinus with hemolysis [10]. Paranasal sinuses involvement by CG seems to be a very rare event. Up today, no one case of CG location in the nasopalatine duct has been reported in literature. Complete excision with Cadwell-Luc procedure or endoscopic tecniques could be perfomed for the treatment of maxillary sinus CG [11]. Recurrence for maxillary sinus CG is not very frequent, with a ratio of about 9,52% (2/21) [9]. In the case reported in this paper, the radiological and clinical features of the lesion simulated another kind of disease, like: nasopalatine duct cyst or others odontogenic lesions. Tc imaging revealed a large erosion of the palatal bone cortex but not a presence of root resorption. For this reason the lesion simulated an inflammatory radicular cyst, although the cortical erosion was very strong. During the surgical operation surgeons noticed a light yellow color of the lesion probably due to the microscopic presence of cholesterol clefts. Because of the similarity with a radicular cyst, and for the presence of cortical palatal erosion we decided to perform a intraoral approach for the excision of the lesion. During the surgical excision we noticed that the apex of the lesion was not in contact with the CG, so we decided to not cut the apex of the tooth. After one year of follow-up no evidences of relapse have been noticed.
Conclusions
CG is a foreign body reaction due to to the deposition of cholesterol crystals in the connective tissues. CG could be found in many anatomic sites of the human body. CG localization in the maxillary area is not very frequent; however in these sites it could simulate other common pathologies. As reported in this paper the localization in the nasopalatine duct could lead to erosion of the palatal bone cortex and simulate more common pathologies. So, CG should be included in the differential diagnosis of lesions arising in the palatine duct and a careful histopathological examination is critical for a correct diagnosis.
References
- Falci SG, Verli FD, Consolaro A, Santos CR (2013) Morphological characterization of the nasopalatine region in human fetuses and its association to pathologies. J Appl Oral Sci 21: 250-255. [Crossref]
- Johnson NR, Batstone MD, Savage NW (2013) Management and recurrence of keratocysticodontogenictumor: a systematic review. Oral Surg Oral Med Oral Pathol Oral Radiol 116: e271-276. [Crossref]
- Tsuneki M, Maruyama S, Yamazaki M, Abé T, Adeola HA, et al. (2013) Inflammatoryhistopathogenesis of nasopalatine duct cyst: a clinicopathological study of 41 cases. Oral Dis 19: 415-424. [Crossref]
- Suter VG, Warnakulasuriya S, Reichart PA, Bornstein MM (2015) Radiographic volume analysis as a novel tool to determine nasopalatine duct cyst dimensions and its association with presenting symptoms and postoperative complications. Clinical Oral Investig 19: 1611-1618. [Crossref]
- Almada CB, Fonseca DR, Vanzillotta RR, Pires FR (2008) Cholesterol granuloma of the maxillary sinus. Braz Dent J 19: 171-174. [Crossref]
- Durgam A, Batra PS (2013)Paranasal sinus cholesterol granuloma: systematic review of diagnostic and management aspects. Int Forum Allergy Rhinol 3: 242-247. [Crossref]
- Bella Z, Torkos A, Tiszlavicz L, Ivan L, Jori J (2005) Cholesterol granuloma of the maxillary sinus resembling an invasive, destructive tumor. Eur Arch Otorhinolaryngol 262: 531-533. [Crossref]
- Ko MT, Hwang CF, Kao YF, Lui CC, Huang CC, et al. (2006) Cholesterol granuloma of the maxillary sinus presenting as sinonasal polyp. Am J Otolaryngol 27: 370-372. [Crossref]
- Chao TK (2006) Cholesterol granuloma of the maxillary sinus. Eur Arch Otorhinolaryngol 263: 592-597.
- Milton CM, Bickerton RC (1986) A review of maxillary sinus cholesterol granuloma. Br J Oral Maxillofac Surg 24: 293-299. [Crossref]
- Marks SC, Smith DM (1995) Endoscopic treatment of maxillary sinus cholesterol granuloma. Laryngoscope 105: 551-552. [Crossref]