Abstract
Introduction
Crohn’s disease is a chronic transmural inflammation the gastrointestinal tract. Commonly develops in the terminal ileum and the proximal colon. It may be presented with unusual presentation which may lead to misdiagnosis as in the current case.
Case report
A 40 year old female patient complaining of fresh rectal bleeding comes either with defecation or as a spotting of fresh blood associated with a difficulty, straining during defecation with stenosis in rectal sphincter and lower back pain associated with skin tags with remission and relapses for 17 years. Ileo-colonscopy reveal marked granular mucosa with loss of normal vascular pattern and multiple scattered aphthloid ulcers in terminal ileum. Histopathology reveal active Crhon's disease. CT features suggestive of active ileal inflammatory bowel disease; Crhon's disease. MRI noted two inter-shincteric fistulous tracts "St-James type I' with high fecal calprotectin.
Conclusion
miss-diagnoses of the present case of Crohn's disease was due to the presence of skin tags that were confused with hemorrhoids. A careful examination of these skin tags is essential for accurate diagnosis. Correlation with other parameters for diagnosing Crhon's disease; ileocolonoscopy and histopatholgical examination correlated with preliminary laboratory data and imaging.
Key words
Crohn's disease (CD), fistula, skin tags, ileocolonoscopy, fecal calprotectin
Introduction
Cohn's disease (CD) is an inflammatory bowel (IBD) of multifactorial etiology, which can strike anywhere from mouth to anus [1]. The disease can then be triggered by any of a number of different unknown environmental factors and sustained by an abnormal immune response to these factors [2]. CD can affect multiple parts of the GI tract simultaneously causing disconnected patches of ulceration between healthy mucosal areas to create a cobblestone appearance. It most commonly develops in the terminal ileum (also called regional enteritis) and the proximal colon (also called granulomatous colitis), extends through all bowel tissue layers, and can penetrate extraintestinal structures [3]. The clinical presentation of CD patients depends on the affected area in the GI tract and it varies from chronic diarrhea, vomiting, abdominal pain to Rectal bleeding, abdominal mass and malnutrition. Sometimes the disease may be presented by unusual presentation which may lead to misdiagnosis as in the current case. Crohn's disease is a challenging disease and sometimes it is difficult to make an accurate diagnosis of this disease; the diagnosis of Crohnʼs disease is based on clinical presentation, evaluation of the entire intestinal tract, and histopathologic findings [4]. A treatment plan should be organized according to disease activity [2], behavior and localization of disease, and associated complications. Whatever treatment plan is chosen, it is most appropriate [5].
Case report
A 40 year old female patient complaining of fresh rectal bleeding that comes either with defecation or as a spotting of fresh blood associated with a difficulty, straining during defecation and a stenosis in rectal sphincter with lower back pain for one year and multiple skin tags in anal verge. During this year, she visited a surgical consultant and two sessions for dilatation of the anal sphincter were performed. There was no improvement in her condition and the case was diagnosed as external and internal piles associated with multiple internal fissures.
She re-presented to a surgeon who noted that the complaint was started 17 years ago. Two Hemoroiectomy operations were done. During this period the patient had multiple remissions and relapses during the course of the disease. A past history of fundoplication and total vagotomy for hiatal hernia and acidic reflux; in addition to antrectomy and gastrojejunostomy (Roux-en-Y anastomosis for duodenal ulcers). Over a period of sixteen years; the patient had frequent rectal bleeding, difficulty during defecation and crampy abdominal pain with steatorrhea. Full lab investigation was performed; fecal calprotectin, liver and kidney function, CBC, in addition to rectal colonoscope till terminal ileum was done which revealed active Crhon's disease; CT with contrast to abdomen and pelvis revealed stenosis with desquamation in terminal ileum associated with colitis. MRI indicated two enteric fistulae. The condition becomes stationary for one year under the treatment with Infliximab (Remicade) injection every two months. One year later Infliximab was stopped and shift the course of treatment to oral Azathioprine tab twice a day. The patient presented to gastroenterology clinic complaining of severe rectal bleeding with and without defecation, lower back pain and anal stenosis. The course of treatment was started again after diagnosing it as relapsing Crhon's disease; Adalimumab (Hummerra 40 mg) subcutaneous injection every two weeks were recommended with other oral medications. Ileo-colonoscopy was done after digital rectal examination and IV sedating the patient under direct vision up to terminal ileum was done twice to the patient first for diagnosis and second one for follow up. Excisional biopsy for sessile polyp and multiple biopsy specimens for entire colonic mucosa and was sent for histopathological assessment.
Multiple specimens from the entire colonic mucosa and from the sessile polyp were fixed on formaline. 4- micron thick recuts of all the formalin-fixed and Haematoxylin-Eosin (H& E) stained sections and were reviewed. CT abdomen and entero-colonography was done also first to assess and diagnose Crhon's disease and second one for follow up. MRI pelvis for perianal fistula was done three times (for diagnosing presence of fistula and for follow up).
Laboratory investigation screening for complete blood picture, liver function, kidney function and fecal calprotectin to correlate significantly with histologic and endoscopic assessment for disease activity.
Results
First result of ileo-colonscopy reveal marked granular mucosa with loss of normal vascular pattern and multiple scattered aphthloid ulcers in terminal ileum. Normal entire colonic mucosa, normal vascular pattern, no ulcers, or masses. A sessile polyp was noted 20 cm from anal verge; impressing Crhon's ileitis. Follow up ileo-colonscopy after one year from starting Infliximab, terminal ileum as well as entire colon had normal looking mucosa. With normal vascular pattern and no masses were seen.
Histopathology report showed areas of chronic inflammation, comprising increased lamina propria plasma cells and lymphocytes, in association with chronic architectural distortion. Note the presence of granuloma and surface ulcer (Figures 1a & b).
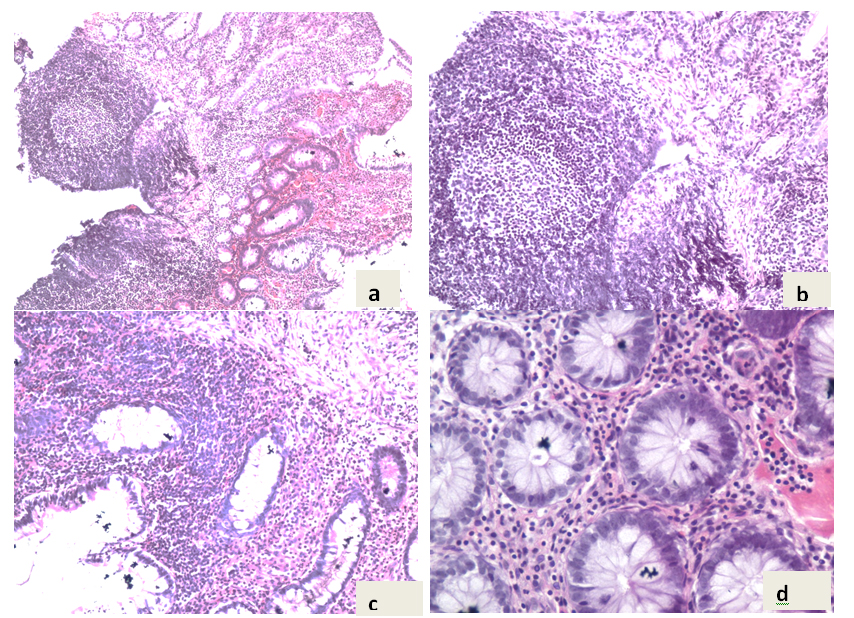
Figure 1. a,b & c) pathological aspect (Hematoxilin–Eosin stain, ×10); d) (HE stain, ×100).
Higher power view demonstrates the presence of dense lymphoplasmacytic infiltrate and the characteristic granuloma, which is formed of histiocytes and lymphocytes. Focally, some glands exihibt low grade atypia, in the form of decreased mucin content, enlarged hyperchromatic nuclei and increased mitosis with abnormal mitotic figures (Figures 1c & d).
CT abdomen and entereo-colonography to assess diagnosis revealed features suggestive of active ileal inflammatory bowel disease; Crhon's disease in the form of transmural thickening of terminal ileum reaching 5 mm displaying mural stratification (mucosal hyper-enhancement, submucosal edema as well as serosal hyper-enhancement) which was the target sign, associated with inflammatory stenosis, mildly prominent vasa recta with regional inflammatory adenopathy.
In the follow up CT abdomen and entereo-colonography normal CT features of the different small and large intestinal loops, with no abnormal enhancement, mural thickening or peri-intestinal mesenteric lesions.
MRI for the first time noted two inter-shincteric fistulous tracts "St-James type I'. Second one after6 month from starting treatment noted short simple inter-shincteric fistula "St-James type I". 6 months later for follow up no MRI evidences of perianal fistulations detected; good improvement of the condition which was correlated with clinical signs and symptoms, CT results and lab investigations.
Discussion
Crohn's disease is a chronic inflammatory bowel disease with remitting and relapsing episodes. It is characterized by the fact that it almost always involves ileum, often has skip lesions, & often colon may be involved [1]. Patients with Crohn's disease always present with symptoms due to the intestinal lesions-diarrhoea and abdominal pain.
Perianal disease, taking the form of deep multiple fissures, undermining anal ulceration, indolent fistula-in-ano, or oedematous skin tags, is known to be common. It is especially likely to complicate Crohn's disease affecting the large bowel [6]; but it may also complicate Crohn's disease otherwise confined to the small intestine. It is important to note that an anal lesion may precede the onset of intestinal symptoms, and this occurred in one-quarter of the cases studied. This was the most obvious symptom in our case that was the most leading cause of being misdiagnosed as Crhon's disease.
To diagnose a case of Crhon's disease the patient should be evaluated initially and symptoms should be elicited in detail. Obtain a complete medical, surgical, social, and family history, and perform a detailed review of systems. Preliminary laboratory data (eg, inflammatory and anemia markers) may be helpful.
Our patient presented with skin tags in anal verge and recurrent profuse rectal bleeding. She had already undergone several investigations in different hospitals, as mentioned previously which led to confusion in diagnosis as she was diagnosed as hemorrhoids. Therefore she was undergo hemorrhoidectomy operation and trials for anal dilatation without any relief of symptoms. Because of this patient sought further medical advice. Considering the history, the gastroenterology doctor reconsidered her diagnosis, re–investigate the patient. It is important here to mention that the patient presented with a rare presenting predominant symptom of Crohn’s disease, in addition to distinct selective involvement of terminal ileum with sparing of colon.
Diagnosis was delayed due to the presence of skin tags in anal verge and colorectal symptoms in the form of rectal bleeding, stenosis and difficulty during defecation and the inability to visualise a enteric fistulas except with MRI pelvis.
To evaluate the disease activity fecal calprotectin have been found to be the most accurate tool to assess the presence of active mucosal inflammation [5]; as compared with clinical scores and common serum markers (ESR, CRP, platelet) and correlated with ileocolonoscopy and other imaging tools [7] .
This might make FC a good biomarker for screening for Crhon's disease or as a noninvasive predictor of increased risk of relapse [8]. In our case fecal calprotectin was a good noninvasive predictor for the disease activity; at time of diagnosis it was 298 mg/kg and after one year under Infliximab the level becomes <45 mg/kg which mean remission of the disease. Other published cases reported that patients who had a calprotectin value >50 mg/L (=250 μg/g) at inclusion were at considerable risk of a relapse during the following year, whereas patients with a calprotectin level <50 mg/L had a good chance to maintain remission [9].
Symptomatic relapse was occurred in the present case in the form of severe rectal bleeding with and without defecation, lower back pain and anal stenosis. This was correlated with fecal calprotectin of 245 mg/kg.
In other previous studies fecal calprotectin do not replace an ileocolonoscopy in the follow up settings in patients with Crohn´s disease. However, a large majority of the patients with calprotectin values below100 μg/g were found to be in ileocolonoscopy remission [9].
Conclusion
In conclusion the miss-diagnoses of the present case of Crohn's disease was due to the presence of skin tags that were confused with hemorrhoids. Anal dilatation of the anal sphincter to relieve the stenosis with different prescribed medications leads to irritation of anal mucosa which was the leading cause crhon's disease activity. So, a careful examination of these skin tags is essential to differentiate between those of Crhon's disease which are generally larger and less tender than hemorrhoids. This must be correlated with other parameters for diagnosing Crhon's disease; ileocolonoscopy and histopatholgical examination correlated with preliminary laboratory data and imaging.
References
- Tillack C, Seiderer J, Brand S, Göke B, Reiser MF, et al. (2008) Correlation of magnetic resonance enteroclysis (MRE) and wireless capsule endoscopy (CE) in the diagnosis of small bowel lesions in Crohn’s disease.Inflamm Bowel Dis14:1219-28. [Crossref]
- Tsianos EV, Katsanos KH, Tsianos VE (2012) Role of genetics in the diagnosis and prognosis of Crohn’s Disease. World J Gastroenterol18: 105-118. [Crossref]
- Baran B, Karaca C (2013) Practical Medical Management of Crohn’s Disease. ISRN Gastroenterol 2013:208073.[Crossref]
- IBD Working Group of the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) (2005) Inflammatory bowel disease in children and adolescents: recommendations for diagnosis - the Porto criteria. J PediatrGastroenterolNutr41:1-7. [Crossref]
- Vrabie R, Kane S (2014) Noninvasive Markers of Disease Activity in Inflammatory Bowel Disease. Gastroenterology &Hepatology 10.
- Baker WN, Milton-Thompson GJ (1971) The anal lesion as the sole presenting symptom of intestinal Crohn's disease. Gut 12: 865.[Crossref]
- Lennard-Jones JE, Shivananda S (1997) Clinical uniformity of inflammatory bowel disease a presentation and during the first year of disease in the north and south of Europe. EC-IBD Study Group. Eur J GastroenterolHepatol 9: 353-359.[Crossref]
- D'Haens G, Ferrante M, Vermeire S, Baert F, Noman M, et al. (2012) Fecal calprotectin is a surrogate marker for endoscopic lesions in inflammatory bowel disease. Inflamm Bowel Dis 18: 2218-2224.[Crossref]
- Lasson A (2014) FecalCalprotectin The usefulness in special clinical situations and issues on the sampling procedure.